You might also like
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Pharmacotherapeutic Management of Cardiovascular Disease Complications: A Textbook for Medical StudentsFrom EverandPharmacotherapeutic Management of Cardiovascular Disease Complications: A Textbook for Medical StudentsNo ratings yet
- Diagnosis and Treatment of Shock: Dr. Refli Hasan SPPD, SPJP (K) FihaDocument37 pagesDiagnosis and Treatment of Shock: Dr. Refli Hasan SPPD, SPJP (K) FihaWinson ChitraNo ratings yet
- Cardiogenic ShockDocument27 pagesCardiogenic ShockMuhammad Ikbar100% (1)
- Shock PathophysiologyDocument63 pagesShock PathophysiologyRani OktasariNo ratings yet
- Shock CorrectedDocument70 pagesShock CorrectedrajevikramNo ratings yet
- Cardiac Tamponade: Pankaj Singh Rana Nurse Practitioner in Critical Care Swami Rama Himalayan UniversityDocument35 pagesCardiac Tamponade: Pankaj Singh Rana Nurse Practitioner in Critical Care Swami Rama Himalayan UniversityBarlonga Yhan YogaNo ratings yet
- Cardiogenic ShockDocument20 pagesCardiogenic ShockMohamed SuhailNo ratings yet
- Cardiogenic Shock: Submitted ToDocument5 pagesCardiogenic Shock: Submitted Toal-obinay shereenNo ratings yet
- Basic Human Needs Oxygenation Ventilation/PerfusionDocument122 pagesBasic Human Needs Oxygenation Ventilation/PerfusionMichael BonillaNo ratings yet
- 4.shock & MonitoringDocument21 pages4.shock & MonitoringDr.G.Bhanu PrakashNo ratings yet
- Shock: Differential Diagnosis and Hemodynamic MonitoringDocument21 pagesShock: Differential Diagnosis and Hemodynamic MonitoringtataranyNo ratings yet
- Handouts in NGCM103 Oxygenation Cardiovascular SystemDocument7 pagesHandouts in NGCM103 Oxygenation Cardiovascular SystemJeenah HannahNo ratings yet
- Case 2 SlosDocument7 pagesCase 2 SlosNamarNo ratings yet
- What Is Cardiogenic Shock?Document3 pagesWhat Is Cardiogenic Shock?nipheyy dananNo ratings yet
- Heart FailureDocument77 pagesHeart FailureJudy Anne PatricioNo ratings yet
- Heart FailureDocument39 pagesHeart FailureMuhammad AsifNo ratings yet
- Cardiac Tamponade and ManagementDocument42 pagesCardiac Tamponade and Managementأم حمدNo ratings yet
- Cardio Notes, Heart FailureDocument17 pagesCardio Notes, Heart FailureJoy DunwanNo ratings yet
- Lec 3Document17 pagesLec 3Yousef El3alamey0% (1)
- MTE Diagnosis and Manag ShockDocument52 pagesMTE Diagnosis and Manag ShockGarbha JmrsNo ratings yet
- ShockDocument49 pagesShockpaulyn ramos100% (1)
- Cardiac EmergencyDocument56 pagesCardiac Emergency21rayhanf100% (1)
- Heart Failure: Mohammad DiahDocument50 pagesHeart Failure: Mohammad DiahAdityaNo ratings yet
- ShockDocument34 pagesShockeman shNo ratings yet
- Cardiogenic ShockDocument31 pagesCardiogenic ShockLovelights ZamoraNo ratings yet
- Cardiopulmonary BypassDocument40 pagesCardiopulmonary BypassParvathy R NairNo ratings yet
- UntitledDocument7 pagesUntitledMAZ OfficialNo ratings yet
- Cardiac Tamponade: Mrs. D.Melba Sahaya Sweety.D M.SC Nursing GimsarDocument23 pagesCardiac Tamponade: Mrs. D.Melba Sahaya Sweety.D M.SC Nursing GimsarD. Melba S.S ChinnaNo ratings yet
- Cardiovascular Assessment & Cardiac DisordersDocument57 pagesCardiovascular Assessment & Cardiac DisordersgtsantosNo ratings yet
- NursingDocument11 pagesNursingfelixlixan100No ratings yet
- Heart Failure: Presentation by Dr. Tooba ShahbazDocument30 pagesHeart Failure: Presentation by Dr. Tooba ShahbazTooba ShahbazNo ratings yet
- CARDIAC FAILURE NewDocument60 pagesCARDIAC FAILURE NewJake MillerNo ratings yet
- Shock: Ron Michael N. Olaguera 2 Year Surgery ResidentDocument40 pagesShock: Ron Michael N. Olaguera 2 Year Surgery ResidentErick Anca100% (2)
- Mnemonic: "D" For "Dilate", and "S" For Bee "Sting"Document6 pagesMnemonic: "D" For "Dilate", and "S" For Bee "Sting"AngelLeeNo ratings yet
- Shock NotesDocument7 pagesShock NotesAnitha NoronhaNo ratings yet
- KGD 1 VivianDocument101 pagesKGD 1 VivianVivian SaputraNo ratings yet
- MEDICAL PATHOLOGIES - CardiovascularDocument6 pagesMEDICAL PATHOLOGIES - Cardiovascularngachangong victorineNo ratings yet
- Heart Failure and ShockDocument34 pagesHeart Failure and Shockfrenee aradanasNo ratings yet
- Cardiogenic Shock Patofisiologi and TreatmentDocument40 pagesCardiogenic Shock Patofisiologi and TreatmentRichi Aditya100% (1)
- Cardiogenic ShockDocument29 pagesCardiogenic ShockagnescheruseryNo ratings yet
- Dr. Az Rifki, Span - Kic Departemen Anestesiologi Dan Reanimasi Rsi Siti Rahmah/Fk-Fkg Universitas Baiturrahmah PadangDocument62 pagesDr. Az Rifki, Span - Kic Departemen Anestesiologi Dan Reanimasi Rsi Siti Rahmah/Fk-Fkg Universitas Baiturrahmah PadangKamelia MarcshendaNo ratings yet
- BIOCHEMISTRY AND PHYSIOLOGY Nuggets PDFDocument137 pagesBIOCHEMISTRY AND PHYSIOLOGY Nuggets PDFHKNo ratings yet
- Shock in The Pediatric Patient: or Oxygen Don't Go Where The Blood Won't Flow!Document63 pagesShock in The Pediatric Patient: or Oxygen Don't Go Where The Blood Won't Flow!Nishanth BabuNo ratings yet
- Cardiogenic ShockDocument27 pagesCardiogenic ShockIgor StefanetNo ratings yet
- General Internal Medicine Hour: HypertensionDocument33 pagesGeneral Internal Medicine Hour: HypertensionRadley Jed C. PelagioNo ratings yet
- Shock Study GuideDocument8 pagesShock Study GuideMadameb1No ratings yet
- Pulmonary EdemaDocument59 pagesPulmonary EdemamaibejoseNo ratings yet
- In Name, There Are Many Doctors, But in Reality Only A FewDocument86 pagesIn Name, There Are Many Doctors, But in Reality Only A FewFalling HateNo ratings yet
- Cardiology Notes by Wasim AhmadDocument28 pagesCardiology Notes by Wasim AhmadAshna moeenNo ratings yet
- Seminar On Blood Pressure: Department of PeriodontologyDocument25 pagesSeminar On Blood Pressure: Department of Periodontologypalak sharmaNo ratings yet
- DR Dhiman BanikCariogenic Shock Final 2022 DDDocument59 pagesDR Dhiman BanikCariogenic Shock Final 2022 DDCloudySkyNo ratings yet
- Seminar On Blood Pressure: Department of PeriodontologyDocument26 pagesSeminar On Blood Pressure: Department of Periodontologypalak sharmaNo ratings yet
- Drugs Acting in CVSDocument63 pagesDrugs Acting in CVSMeghan Norico Cristuta100% (1)
- Kebutuhan Dasar Manusia OksigenasiDocument117 pagesKebutuhan Dasar Manusia Oksigenasiintanputri ramadhaniNo ratings yet
- Cardiogenic Shock: by Fritzanella LafondDocument42 pagesCardiogenic Shock: by Fritzanella LafondhaphahapNo ratings yet
- Circulatory Response To ExerciseDocument31 pagesCirculatory Response To ExerciseFarhad GulNo ratings yet
- Cardiogenic ShockDocument8 pagesCardiogenic ShockMAE RACHELLE LAMOSTENo ratings yet
- Heart Pump and Cardiac Cycle: Faisal I. Mohammed, MD, PHDDocument41 pagesHeart Pump and Cardiac Cycle: Faisal I. Mohammed, MD, PHDUsama SadiqNo ratings yet
- Ipd - KardiologiDocument116 pagesIpd - KardiologiWynda MuljonoNo ratings yet
- Jur Inter Perekaman EKGDocument9 pagesJur Inter Perekaman EKGAyu LuthfiyahNo ratings yet
- Part 4 - Skill 1 - Be Sure S ODocument2 pagesPart 4 - Skill 1 - Be Sure S OAyu LuthfiyahNo ratings yet
- Jurnal 2014-2015 PDFDocument5 pagesJurnal 2014-2015 PDFAiyuNarthaLovenhaAdjehNo ratings yet
- Status Kesehatan FixDocument4 pagesStatus Kesehatan FixAyu LuthfiyahNo ratings yet
- Judul Skripsi Semester Genap Tahun Ajaran 2018 2019 Campus C 15 Maret 2019Document2 pagesJudul Skripsi Semester Genap Tahun Ajaran 2018 2019 Campus C 15 Maret 2019Ayu LuthfiyahNo ratings yet
- GPAQ Analysis GuideDocument23 pagesGPAQ Analysis GuideThe-Queen Wicked-YglesiasNo ratings yet
- 1 SM PDFDocument24 pages1 SM PDFNikita WulanNo ratings yet
- Pengaruh Senam Kaki Diabetik Terhadap Penderita Diabetes Tipe 1Document11 pagesPengaruh Senam Kaki Diabetik Terhadap Penderita Diabetes Tipe 1Ayu LuthfiyahNo ratings yet
- Catatan PerawatanDocument5 pagesCatatan PerawatanAyu LuthfiyahNo ratings yet
- 33 Diagnosis Keperawatan Jiwa NANDADocument2 pages33 Diagnosis Keperawatan Jiwa NANDAaurelia_diandra69% (13)
- Tugas Bahasa Ingrris AyuDocument6 pagesTugas Bahasa Ingrris AyuAyu LuthfiyahNo ratings yet
- Catatan PerawatanDocument5 pagesCatatan PerawatanAyu LuthfiyahNo ratings yet
- TB BB Uk. Sepatu Jarak Ke Kampus Tempat Tinggal Pengeluaran IPKDocument1 pageTB BB Uk. Sepatu Jarak Ke Kampus Tempat Tinggal Pengeluaran IPKAyu LuthfiyahNo ratings yet
- Cardiogenic Shock - SWDocument41 pagesCardiogenic Shock - SWAyu LuthfiyahNo ratings yet
- Pidi Baiq - Dilan-1 PDFDocument333 pagesPidi Baiq - Dilan-1 PDFatika angNo ratings yet
- Penyebab: Apa Itu Demam Berdarah DengueDocument2 pagesPenyebab: Apa Itu Demam Berdarah DengueAyu LuthfiyahNo ratings yet
- Anemia EnglishDocument9 pagesAnemia EnglishAyu LuthfiyahNo ratings yet
- Sop Hand HygieneDocument2 pagesSop Hand HygieneAyu LuthfiyahNo ratings yet
- 2 Marks Q & ADocument11 pages2 Marks Q & AJayaprakash JayaramanNo ratings yet
- StreptokinaseDocument18 pagesStreptokinasedickyNo ratings yet
- Local Anesthesia Exam TipsDocument9 pagesLocal Anesthesia Exam TipsshadapaaakNo ratings yet
- Oral RevalidaDocument3 pagesOral RevalidaJaye DangoNo ratings yet
- Unit 2 Chapter 8 Text For Diff Purposes - Doc 1Document11 pagesUnit 2 Chapter 8 Text For Diff Purposes - Doc 1Seandrae PaeldenNo ratings yet
- Merci Ships Annual Report Cpr-31Document32 pagesMerci Ships Annual Report Cpr-31larryfoleNo ratings yet
- Legal and Ethical Issues-ModifiedDocument29 pagesLegal and Ethical Issues-Modifiedmonir61100% (1)
- Responding To Ten Common Delirium MisconceptionsDocument7 pagesResponding To Ten Common Delirium MisconceptionsFelipe Rangel Hassey100% (1)
- Asthma Case Report FinalDocument6 pagesAsthma Case Report FinalJiaYee GoNo ratings yet
- Article - Quick REMAP - Steps in The Quick REMAP4-point Rapid Relief Protocol 1 PDFDocument32 pagesArticle - Quick REMAP - Steps in The Quick REMAP4-point Rapid Relief Protocol 1 PDFAnonymous g8zT2sPtjW100% (1)
- Blood DetailsDocument13 pagesBlood DetailsKishore Babu PvrNo ratings yet
- Extubation TestDocument5 pagesExtubation TestMel GriffinNo ratings yet
- FenofibrateDocument7 pagesFenofibrateVikas Karande100% (1)
- Clinical Practice Guideline BPPVDocument47 pagesClinical Practice Guideline BPPVAnggaRusdiantoNo ratings yet
- PIID 184 Post Mortem April 17Document7 pagesPIID 184 Post Mortem April 17Rey Loro PongautanNo ratings yet
- Guia Tiva 2018Document14 pagesGuia Tiva 2018John Bryan Herrera DelgadoNo ratings yet
- Pharmacogenomics 121004112431 Phpapp02Document53 pagesPharmacogenomics 121004112431 Phpapp0288AKK100% (1)
- Annexure C: Medical and Dental Professions BoardDocument2 pagesAnnexure C: Medical and Dental Professions BoardK ValdesNo ratings yet
- Annotated BibliographyDocument2 pagesAnnotated Bibliographyapi-237172063No ratings yet
- Total Patient Care Nursing or Case Method NursingDocument3 pagesTotal Patient Care Nursing or Case Method Nursingkint manlangitNo ratings yet
- Effect of Orofacial Myofunctional Exercise Using An Oral Rehabilitation Tool On Labial Closure Strength, Tongue Elevation Strength and Skin ElasticityDocument4 pagesEffect of Orofacial Myofunctional Exercise Using An Oral Rehabilitation Tool On Labial Closure Strength, Tongue Elevation Strength and Skin ElasticityUniversity Malaya's Dental Sciences ResearchNo ratings yet
- Blood Transfusion NotesDocument1 pageBlood Transfusion NotesShreyas WalvekarNo ratings yet
- MastitisDocument13 pagesMastitisapi-232713902No ratings yet
- A Case Presentation On:: Bipolar 1 Disorder, MRE With Psychotic FEARURESDocument57 pagesA Case Presentation On:: Bipolar 1 Disorder, MRE With Psychotic FEARURESLane Mae Magpatoc NoerrotNo ratings yet
- Updates in The Management of Diabetic Ketoacidosis: Kathryn Evans Kreider, DNP, FNP-BCDocument7 pagesUpdates in The Management of Diabetic Ketoacidosis: Kathryn Evans Kreider, DNP, FNP-BCLenin Zavaleta RodriguezNo ratings yet
- Efficacy of Nerve Flossing Technique On Improving Sciatic Nerve Function in Patients With Sciatica - A Randomized Controlled TrialDocument10 pagesEfficacy of Nerve Flossing Technique On Improving Sciatic Nerve Function in Patients With Sciatica - A Randomized Controlled Trialsphadungkit100% (1)
- Nursing Responsibilities For Oxygen AdministrationDocument3 pagesNursing Responsibilities For Oxygen AdministrationJahseh WolfeNo ratings yet
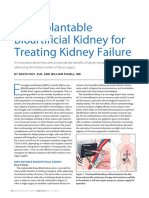
- An Implantable Bioartificial Kidney For Treating Kidney FailureDocument2 pagesAn Implantable Bioartificial Kidney For Treating Kidney FailureAnugrah Pangeran100% (1)
- Case Study HFMD :)Document15 pagesCase Study HFMD :)Princess CavestaniNo ratings yet
- DummyDocument13 pagesDummyShellNo ratings yet