You might also like
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!From EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!No ratings yet
- The Pathophysiology and Pharmacotherapy of Myocardial InfarctionFrom EverandThe Pathophysiology and Pharmacotherapy of Myocardial InfarctionNabil El-SherifNo ratings yet
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsNo ratings yet
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- ECG Interpretation GuideDocument69 pagesECG Interpretation GuideRohini RaiNo ratings yet
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- Cardiovascular Disorders Proper 1232011849539043 1Document111 pagesCardiovascular Disorders Proper 1232011849539043 1api-19824701No ratings yet
- Cardiac Study GuideDocument9 pagesCardiac Study GuideJane DiazNo ratings yet
- Pharmacology RevisedDocument59 pagesPharmacology Revisedjohnstockton12100% (1)
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- Cardiac MedsDocument7 pagesCardiac MedsMary Fair DelcidNo ratings yet
- CRITICAL THINKING IN CLINICAL NURSING PRACTICE (RN): Passbooks Study GuideFrom EverandCRITICAL THINKING IN CLINICAL NURSING PRACTICE (RN): Passbooks Study GuideNo ratings yet
- Complications of Acute Myocardial Infarction (AMIDocument5 pagesComplications of Acute Myocardial Infarction (AMIlourdesfercab_at_msn100% (1)
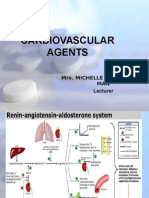
- Cardiovascular Agents: Mrs. Michelle A. Iduria, RN, MAN LecturerDocument131 pagesCardiovascular Agents: Mrs. Michelle A. Iduria, RN, MAN LecturerNiala AlmarioNo ratings yet
- Arterial Lines in PACU: Presented by Autum Jacobs RN, BSNDocument34 pagesArterial Lines in PACU: Presented by Autum Jacobs RN, BSNinuko1212No ratings yet
- Arrhythmias Teacher GuideDocument12 pagesArrhythmias Teacher GuideMayer Rosenberg100% (3)
- Cardiac Nursing II Study GuideDocument6 pagesCardiac Nursing II Study GuiderunnermnNo ratings yet
- Intra Aortic Balloon PumpDocument5 pagesIntra Aortic Balloon PumpZainal 'babeh' Arifin100% (1)
- Cardiac DysrythmiasDocument190 pagesCardiac DysrythmiasKoRnflakes100% (4)
- Managing Cardiac Dysrhythmias and Conduction ProblemsDocument29 pagesManaging Cardiac Dysrhythmias and Conduction ProblemsYlanni Coritana100% (1)
- DYSRHYTHMIASDocument9 pagesDYSRHYTHMIASgudobenNo ratings yet
- Top Nursing Actions for Chest Pain, Transfusions, Evisceration and MoreDocument4 pagesTop Nursing Actions for Chest Pain, Transfusions, Evisceration and MoreAnn ChenNo ratings yet
- Dysrhythmia Instructor 2018 2 PDFDocument105 pagesDysrhythmia Instructor 2018 2 PDFtvrossyNo ratings yet
- Intravenous Medication Care and ComplicationDocument42 pagesIntravenous Medication Care and Complicationtummalapalli venkateswara rao100% (2)
- Selected Nursing Diagnoses and Interventions For Patients With DysrhythmiasDocument19 pagesSelected Nursing Diagnoses and Interventions For Patients With Dysrhythmiaslanie_jecielNo ratings yet
- HeartFailure Nursing FIK 2014Document101 pagesHeartFailure Nursing FIK 2014Putri NurlaeliNo ratings yet
- CardiopathophysiologyDocument63 pagesCardiopathophysiologyapplesncoreNo ratings yet
- Cardiac CatheterizationDocument3 pagesCardiac CatheterizationAmir ZiadNo ratings yet
- Common Cardiac MedicationsDocument1 pageCommon Cardiac MedicationsPaige HardekopfNo ratings yet
- Mechanical Ventilation For NursingDocument55 pagesMechanical Ventilation For NursingAmira AttyaNo ratings yet
- Cardiomyopathy Joisy AloorDocument31 pagesCardiomyopathy Joisy AloorJoisy AloorNo ratings yet
- Safe and Effective Care EnvironmentDocument8 pagesSafe and Effective Care Environmentgretch_carreonNo ratings yet
- Antiarrhythmic Agents Lecture NotesDocument6 pagesAntiarrhythmic Agents Lecture NotesErnest Patrick MatiasNo ratings yet
- Basis of ECG and Intro To ECG InterpretationDocument10 pagesBasis of ECG and Intro To ECG InterpretationKristin SmithNo ratings yet
- Cardiac pacing guide for beginnersDocument89 pagesCardiac pacing guide for beginnerssandwhale056No ratings yet
- Cardiovascular SYSTEM - Heart Dysrythmia IllustrationsDocument3 pagesCardiovascular SYSTEM - Heart Dysrythmia IllustrationsKim GonzalesNo ratings yet
- EKG Basics1Document16 pagesEKG Basics1Jamie Lemons100% (1)
- Diagnosis of Cardiovascular Disease - TranscriptionDocument11 pagesDiagnosis of Cardiovascular Disease - TranscriptionPauline Del MundoNo ratings yet
- Ecg StripsDocument39 pagesEcg StripsNursyNurse100% (3)
- This Study Resource Was Shared Via: Sinus BradycardiaDocument3 pagesThis Study Resource Was Shared Via: Sinus BradycardiaPascal St Peter NwaorguNo ratings yet
- Cardiac Medications:: What's With The Mixing & Matching?Document97 pagesCardiac Medications:: What's With The Mixing & Matching?TinaHoNo ratings yet
- Clinical KardexDocument2 pagesClinical KardexJackie Frey100% (2)
- Nursing Responsibilities For The Patient Will Undergo Cardiac CatheterizationDocument4 pagesNursing Responsibilities For The Patient Will Undergo Cardiac CatheterizationCharlene Jacobe Cornista100% (1)
- Cardiac Physiology PDFDocument17 pagesCardiac Physiology PDFAli Aborges Jr.No ratings yet
- My Cheat SheetDocument3 pagesMy Cheat SheetTenzin KyizomNo ratings yet
- Types and Management of Valvular Heart DiseaseDocument60 pagesTypes and Management of Valvular Heart DiseaseIntan Kumalasari RambeNo ratings yet
- Mnemonics PDFDocument15 pagesMnemonics PDFbeingfiredNo ratings yet
- Ecg InterpretationDocument9 pagesEcg InterpretationEthan Rodriguez100% (3)
- ECG and ArrhythmiasDocument25 pagesECG and ArrhythmiasRashed ShatnawiNo ratings yet
- Cardiac DisordersDocument80 pagesCardiac Disordersscan1993No ratings yet
- IV PDFDocument63 pagesIV PDFelbagouryNo ratings yet
- Inotropes, Excellent Article, With DosingDocument47 pagesInotropes, Excellent Article, With DosingNavojit ChowdhuryNo ratings yet
- Concept Map 1Document5 pagesConcept Map 1api-396919069No ratings yet
- Management of ArrhythmiasDocument4 pagesManagement of ArrhythmiasAray Al-AfiqahNo ratings yet
- Treating patients with various medical conditionsDocument15 pagesTreating patients with various medical conditionsHafidh Alyza RNo ratings yet
- Case Study - Congestive Heart FailureDocument71 pagesCase Study - Congestive Heart FailureFrancis Adrian100% (3)
- Endocrine System - Part 2Document31 pagesEndocrine System - Part 2Maryem NabawiNo ratings yet
- Trastornos Del Lenguaje MB 7DS.008.1Document48 pagesTrastornos Del Lenguaje MB 7DS.008.1Ruth VegaNo ratings yet
- Treatment of Pituitary Adenoma by Traditional Medicine TherapiesDocument3 pagesTreatment of Pituitary Adenoma by Traditional Medicine TherapiesPirasan Traditional Medicine CenterNo ratings yet
- Manual Urinary SystemDocument6 pagesManual Urinary Systemrayverjohnlayam073No ratings yet
- Renal Histology Biolucida AnswersDocument6 pagesRenal Histology Biolucida Answersjhk0428No ratings yet
- Abscess With Bioprosthetic ValveDocument2 pagesAbscess With Bioprosthetic ValveChalikias GeorgeNo ratings yet
- Renal Clearance 2Document3 pagesRenal Clearance 2Ine Marthia DanieNo ratings yet
- Sensory Processes and Perception ChapterDocument6 pagesSensory Processes and Perception ChapterTaima TarabishiNo ratings yet
- Physiology Practical 2: Toad HeartDocument10 pagesPhysiology Practical 2: Toad HeartAdams OdanjiNo ratings yet
- Chapter4 Biol102 at 31-10-2016Document66 pagesChapter4 Biol102 at 31-10-2016Abdulaziz AHNo ratings yet
- Biology Assignment 2 Atefah Razack 1Document15 pagesBiology Assignment 2 Atefah Razack 1api-491258706No ratings yet
- My Small and Large Intestines: © Teacher Created Resources, Inc. #211 My BodyDocument3 pagesMy Small and Large Intestines: © Teacher Created Resources, Inc. #211 My Bodyalana reneNo ratings yet
- From Cell To OrganismDocument8 pagesFrom Cell To OrganismSheryl BorromeoNo ratings yet
- Cellular Adaptation To Stress:: - Hyperplasia - Hypertrophy - Atrophy - Metaplasia - DysplasiaDocument38 pagesCellular Adaptation To Stress:: - Hyperplasia - Hypertrophy - Atrophy - Metaplasia - DysplasiaRjDNo ratings yet
- GEN - US Dilated Renal Pelvis Handout - tcm63-9940Document2 pagesGEN - US Dilated Renal Pelvis Handout - tcm63-9940Christina Manguiob EscasinasNo ratings yet
- Capitol Medical Center Specialists GuideDocument3 pagesCapitol Medical Center Specialists GuideRonald VillarazaNo ratings yet
- Human Biology: Unit PaperDocument28 pagesHuman Biology: Unit PaperNang Seng Tawng HparawNo ratings yet
- Detailed Lesson Plan in Science 7Document8 pagesDetailed Lesson Plan in Science 7Maeflor AdolfoNo ratings yet
- Neurons and Glial Cells: Structure and FunctionsDocument59 pagesNeurons and Glial Cells: Structure and FunctionsMelissa Aina Mohd YusofNo ratings yet
- Day 6 Urogenital System: Identifying Organs of the Urinary and Reproductive SystemsDocument12 pagesDay 6 Urogenital System: Identifying Organs of the Urinary and Reproductive SystemsChristine BarongoNo ratings yet
- THE Process of DigestionDocument39 pagesTHE Process of DigestionskaiiNo ratings yet
- Final Exam Review - Bio 172Document21 pagesFinal Exam Review - Bio 172Erin McElhaney QuirkNo ratings yet
- PancreasDocument6 pagesPancreasSimran Radhika JasujaNo ratings yet
- Final Hydrocephalus Care PlanDocument11 pagesFinal Hydrocephalus Care PlanSAYMABANUNo ratings yet
- NEUROANATOMY MCQ's Summer 2004Document2 pagesNEUROANATOMY MCQ's Summer 2004i can always make u smile :DNo ratings yet
- Thyroid Disorder PDFDocument324 pagesThyroid Disorder PDFdhilsss nabNo ratings yet
- Chapter 13 - Nervous System in Mammals IDocument54 pagesChapter 13 - Nervous System in Mammals Iapi-3728508100% (2)
- 12 Protection Support and Movement 1Document9 pages12 Protection Support and Movement 1Raiden EiNo ratings yet