You might also like
- Enema AdministrationDocument37 pagesEnema Administrationapi-3722454100% (6)
- Enema AdministrationDocument81 pagesEnema Administrationسانو روديل100% (11)
- Skills Enema AdministrationDocument16 pagesSkills Enema AdministrationFreida Michelle BonnitNo ratings yet
- EnemaDocument6 pagesEnemaKim Lloyd Tensuan Ong100% (1)
- Enema PowepointDocument17 pagesEnema PowepointShane Lim Garcia0% (1)
- Administering An EnemaDocument2 pagesAdministering An EnemaMichael SilvaNo ratings yet
- Hot Sitz Bath: Elaine Frances M. Illo, R.M., R.NDocument17 pagesHot Sitz Bath: Elaine Frances M. Illo, R.M., R.NElaine Frances IlloNo ratings yet
- EnemaDocument16 pagesEnemaFil AquinoNo ratings yet
- Enema PresentationDocument34 pagesEnema PresentationVishalni Menon Returnz100% (2)
- Basic Ostomy CareDocument5 pagesBasic Ostomy CareNathalie Faith CotengNo ratings yet
- Perineal CareDocument7 pagesPerineal CareAna Maria Teresa H RollanNo ratings yet
- SituationdDocument64 pagesSituationdIvory SantiagoNo ratings yet
- Heat and Cold ApplicationDocument95 pagesHeat and Cold Applicationaibuty100% (7)
- 3 Surgical Asepsis PDFDocument32 pages3 Surgical Asepsis PDFLimYiNo ratings yet
- Ante, Intra, PostpartumDocument64 pagesAnte, Intra, PostpartumJaypee Fabros EdraNo ratings yet
- Bedpan or A Urinal: What You Need To Know: What Are Bedpans and Urinals?Document8 pagesBedpan or A Urinal: What You Need To Know: What Are Bedpans and Urinals?Shereen AlobinayNo ratings yet
- Enema 2Document6 pagesEnema 2Muhammad Shafiullah100% (1)
- Intrapartum 111: 1. Examine The Woman For Emergency SignsDocument7 pagesIntrapartum 111: 1. Examine The Woman For Emergency SignsJane MartinNo ratings yet
- Arellano University - Funda Reviewer - 1Document11 pagesArellano University - Funda Reviewer - 1tinea nigraNo ratings yet
- Cricothyroidotomy and Needle CricothyrotomyDocument10 pagesCricothyroidotomy and Needle CricothyrotomyDANDYNo ratings yet
- Nursing Care of The NewbornDocument86 pagesNursing Care of The Newbornjapzee1988100% (1)
- EnemaDocument10 pagesEnemaYolly Tayco Baclayon CaiNo ratings yet
- Oral Rehydration TherapyDocument17 pagesOral Rehydration TherapyJaya PrabhaNo ratings yet
- Enema 2Document34 pagesEnema 2knotstm100% (1)
- Obstetrical Emergency & ManagementDocument38 pagesObstetrical Emergency & ManagementDrPreeti Thakur ChouhanNo ratings yet
- Postpartum AssessmentDocument3 pagesPostpartum AssessmentgirishNo ratings yet
- Urinary Catherization ProcedureDocument12 pagesUrinary Catherization Procedurealbert manievoNo ratings yet
- Engorgement Post Partum: Merry C.ODocument12 pagesEngorgement Post Partum: Merry C.OmerycoNo ratings yet
- PDF Enema Administration ChecklistDocument4 pagesPDF Enema Administration ChecklistALYNo ratings yet
- Enema Procedure: Program Studi Ilmu Keperawatan Stikes Wira Medika Ppni Bali TAHUN 2014/2015Document3 pagesEnema Procedure: Program Studi Ilmu Keperawatan Stikes Wira Medika Ppni Bali TAHUN 2014/2015Putu MitaNo ratings yet
- FC Insertion and RemovalDocument30 pagesFC Insertion and RemovalAngel Alexa Del MundoNo ratings yet
- Stages of LaborDocument30 pagesStages of LaborPerrilyn Perey100% (1)
- Perineal Care Procedure ChecklistDocument3 pagesPerineal Care Procedure ChecklistMarku LeeNo ratings yet
- ST ND RDDocument12 pagesST ND RDwaterbuglilyNo ratings yet
- Collection of Clean Catch Urine SpecimenDocument21 pagesCollection of Clean Catch Urine Specimendeonrey1989100% (1)
- EnemaDocument2 pagesEnemabhabydmcheNo ratings yet
- Bowel and Bladder EliminationDocument9 pagesBowel and Bladder EliminationApril Urbano-Gabot Alap0% (1)
- NCM QuizDocument7 pagesNCM QuizKyla Marie NabongNo ratings yet
- Checkist For NCM 100 (Skills)Document35 pagesCheckist For NCM 100 (Skills)RazelAnneValinoNo ratings yet
- Ob - Abnormalities of The Third Stage of Labor andDocument108 pagesOb - Abnormalities of The Third Stage of Labor andapi-3856051100% (2)
- Checklist On Administering Cleansing Enema: ProcedureDocument3 pagesChecklist On Administering Cleansing Enema: ProcedureKyla CalzadoNo ratings yet
- Note PediaDocument4 pagesNote PediaJAMES ROD MARINDUQUENo ratings yet
- Hot Sitz Bath Nursing Interventions & Procedure: Raymark G. Barredo, RN, RM, MANDocument17 pagesHot Sitz Bath Nursing Interventions & Procedure: Raymark G. Barredo, RN, RM, MANVirgie Lastrollo MoraldeNo ratings yet
- How To Do Tepid Sponge Bath: InstructionsDocument2 pagesHow To Do Tepid Sponge Bath: Instructionssuandi isindaNo ratings yet
- Oleh: Nina Gartika, M.KepDocument41 pagesOleh: Nina Gartika, M.KepAgnisa HayatiNo ratings yet
- Types of Drug Preparation (Credit To The Rightful Owner)Document1 pageTypes of Drug Preparation (Credit To The Rightful Owner)Keren Grace EspirituNo ratings yet
- Practice Drill For Partograph Case ScenarioDocument2 pagesPractice Drill For Partograph Case ScenarioBethrice MelegritoNo ratings yet
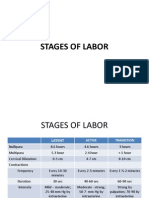
- First Stage: Stages of Labor Start End Duration Nullipara MultiparaDocument4 pagesFirst Stage: Stages of Labor Start End Duration Nullipara MultiparaElleNo ratings yet
- Ob MaternityDocument46 pagesOb MaternityJohanna Erazo Padilla100% (1)
- PostpartumDocument8 pagesPostpartumStudent NurseNo ratings yet
- NCM-N107 Growth and DevelopmentDocument147 pagesNCM-N107 Growth and DevelopmentInsatiable CleeNo ratings yet
- High - Risk PregnancyDocument110 pagesHigh - Risk PregnancyAndre DityaNo ratings yet
- Power Git EndoDocument170 pagesPower Git Endoapi-3735995100% (1)
- 5 P - S of LaborDocument19 pages5 P - S of LaborPerrilyn PereyNo ratings yet
- NCM 109 Skills ChecklistDocument8 pagesNCM 109 Skills ChecklistReygine CariñoNo ratings yet
- Discharge PlanningDocument2 pagesDischarge PlanningAthena Irish LastimosaNo ratings yet
- Newborn Resuscitation ChecklistDocument58 pagesNewborn Resuscitation Checklistboinkjilijoy50% (2)
- Assessment:: Breast & AxillaeDocument96 pagesAssessment:: Breast & Axillaeafreenbegum-0502No ratings yet
- EnemaDocument2 pagesEnemaMelanie ZoiloNo ratings yet
- The Thorax and Lungs Assessment (Autosaved)Document49 pagesThe Thorax and Lungs Assessment (Autosaved)Arlyn Mendenilla100% (4)
- Principles of Drug AdministrationDocument34 pagesPrinciples of Drug AdministrationArlyn Mendenilla100% (1)
- Common Diagnolastic ProceduresDocument151 pagesCommon Diagnolastic ProceduresArlyn MendenillaNo ratings yet
- Assessment of The BreastDocument14 pagesAssessment of The BreastArlyn MendenillaNo ratings yet
- Assessing The Ear and HearingDocument32 pagesAssessing The Ear and HearingArlyn Mendenilla0% (1)
- Assessing The Ear and HearingDocument32 pagesAssessing The Ear and HearingArlyn MendenillaNo ratings yet
- II.C. Data Processing-InternetDocument19 pagesII.C. Data Processing-InternetArlyn MendenillaNo ratings yet
- Surgical AsepsisDocument40 pagesSurgical AsepsisArlyn Mendenilla100% (1)
- The Thorax and Lungs Assessment (Autosaved)Document49 pagesThe Thorax and Lungs Assessment (Autosaved)Arlyn Mendenilla67% (3)
- AnemiaDocument31 pagesAnemiaXunaira AliNo ratings yet
- Respiratory System DrugsDocument64 pagesRespiratory System DrugsArlyn MendenillaNo ratings yet
- Hhns CabaisDocument34 pagesHhns CabaisArlyn Mendenilla100% (1)
- Assessment of The EyesDocument32 pagesAssessment of The EyesArlyn Mendenilla100% (1)
- Tube FeedingDocument47 pagesTube FeedingArlyn Mendenilla0% (1)
- Common Diagnolastic ProceduresDocument151 pagesCommon Diagnolastic ProceduresArlyn MendenillaNo ratings yet
- Dengue FeverDocument33 pagesDengue FeverArlyn MendenillaNo ratings yet
- Charting: Prepared By: Amelia Filio Nacario R.N. MANDocument38 pagesCharting: Prepared By: Amelia Filio Nacario R.N. MANArlyn MendenillaNo ratings yet
- CBR Bahasa Inggris Fisika Kelompok 1Document9 pagesCBR Bahasa Inggris Fisika Kelompok 1Ryan SianiparNo ratings yet
- 3 Speed and AgilityDocument37 pages3 Speed and Agilitymartimparreira69No ratings yet
- Complete Wedding With DJ Worksheets.4pgsDocument4 pagesComplete Wedding With DJ Worksheets.4pgsDanniNo ratings yet
- Case MyelitisDocument34 pagesCase Myelitisyolanda nurlizaNo ratings yet
- Factors Influencing The PerceptionDocument1 pageFactors Influencing The PerceptionTinesh Kumar100% (1)
- Steel Gables and Arches PDFDocument52 pagesSteel Gables and Arches PDFMonny MOM100% (1)
- Breast Stimulation Susilowati 2004138Document11 pagesBreast Stimulation Susilowati 2004138Ahmad SaifuddinNo ratings yet
- Executive ReportDocument51 pagesExecutive ReportPrecelle Joy YangaNo ratings yet
- Theri GathaDocument26 pagesTheri GathaLalit MishraNo ratings yet
- Cisco SF300Document401 pagesCisco SF300Rodney PolingNo ratings yet
- G12 Folk DanceDocument30 pagesG12 Folk DanceTremolo backNo ratings yet
- G.R. No. 92735 Monarch V CA - DigestDocument2 pagesG.R. No. 92735 Monarch V CA - DigestOjie Santillan100% (1)
- BM AssignmentDocument7 pagesBM AssignmentAntony LawrenceNo ratings yet
- Re-Evaluation of DNV Simplified Formulae For Crane Tip MotionsDocument10 pagesRe-Evaluation of DNV Simplified Formulae For Crane Tip Motionsguxiaom100% (1)
- Project SelectingDocument29 pagesProject SelectingayyazmNo ratings yet
- Classical Vs KeynisianDocument8 pagesClassical Vs KeynisianRinky BhattacharyaNo ratings yet
- Lecture05e Anharmonic Effects 2Document15 pagesLecture05e Anharmonic Effects 2Saeed AzarNo ratings yet
- Aja052550590 786Document13 pagesAja052550590 786EugeneSeasoleNo ratings yet
- Thesis Report On: Bombax InsigneDocument163 pagesThesis Report On: Bombax InsigneShazedul Islam SajidNo ratings yet
- Hierarchy Weber and The Old ModelDocument24 pagesHierarchy Weber and The Old ModelDragos XpeNo ratings yet
- National Social Protection Strategy GhanaDocument95 pagesNational Social Protection Strategy GhanaSisiraPinnawalaNo ratings yet
- Best Management of Irritable Bowel SyndromeDocument13 pagesBest Management of Irritable Bowel SyndromeIsaac Martinez ArevaloNo ratings yet
- State MottosDocument3 pagesState MottosFrancisco MedinaNo ratings yet
- IA Feedback Template RevisedDocument1 pageIA Feedback Template RevisedtyrramNo ratings yet
- After The Banquet - Yukio MishimaDocument171 pagesAfter The Banquet - Yukio Mishimalazar10plusNo ratings yet
- Buad 306 HW 2Document4 pagesBuad 306 HW 2AustinNo ratings yet
- Gender Roles As Seen Through Wedding Rituals in A Rural Uyghur Community, in The Southern Oases of The Taklamakan Desert (#463306) - 541276Document26 pagesGender Roles As Seen Through Wedding Rituals in A Rural Uyghur Community, in The Southern Oases of The Taklamakan Desert (#463306) - 541276Akmurat MeredovNo ratings yet
- Purification and Detection of Linamarin From Cassava Root Cortex by HPLCDocument5 pagesPurification and Detection of Linamarin From Cassava Root Cortex by HPLCJohn Eiver BelalcazarNo ratings yet
- How Emotionally Intelligent Are You Wong and Law Emotional Intelligence Scale WLEISDocument2 pagesHow Emotionally Intelligent Are You Wong and Law Emotional Intelligence Scale WLEISIsabela Bică100% (2)