You might also like
- 432 HZ - Unearthing The Truth Behind Nature's FrequencyDocument6 pages432 HZ - Unearthing The Truth Behind Nature's FrequencyShiv KeskarNo ratings yet
- TB in The WorkplaceDocument60 pagesTB in The Workplacemefav7778520100% (1)
- Project Execution PlanDocument69 pagesProject Execution PlanGraco Calle100% (6)
- Manual de Servicio CX 350B 84355067-Dmc Site OnlyDocument127 pagesManual de Servicio CX 350B 84355067-Dmc Site Onlyabel jairo santos cabello100% (2)
- House OfficerDocument32 pagesHouse Officerapi-3705046100% (1)
- House OfficerDocument32 pagesHouse Officerapi-3705046100% (1)
- Sample Behavioral Interview QuestionsDocument3 pagesSample Behavioral Interview QuestionssanthoshvNo ratings yet
- Abdominal Pain in PregnancyDocument22 pagesAbdominal Pain in Pregnancyapi-3705046No ratings yet
- Dysfunctional Uterine Bleeding (DUB)Document21 pagesDysfunctional Uterine Bleeding (DUB)api-3705046100% (2)
- ContraceptionDocument39 pagesContraceptionapi-3705046100% (3)
- CPG Management of Type 2 Diabetes Mellitus (5th Edition) Special AFES Congress EditionDocument141 pagesCPG Management of Type 2 Diabetes Mellitus (5th Edition) Special AFES Congress Editionkhangsiean89100% (1)
- Sickle Cell Disease in PregnancyDocument18 pagesSickle Cell Disease in Pregnancyapi-370504667% (3)
- ABAP Performance Tuning Tips and TricksDocument4 pagesABAP Performance Tuning Tips and TricksEmilSNo ratings yet
- Rhesus Iso ImmunizationDocument12 pagesRhesus Iso Immunizationapi-3705046No ratings yet
- Membrane TypesDocument92 pagesMembrane TypesVanditaa Kothari100% (1)
- Evolving Roles of Pharmacists in AMS by Dr. Mediadora SanielDocument72 pagesEvolving Roles of Pharmacists in AMS by Dr. Mediadora SanielMark Anthony EllanaNo ratings yet
- Structured Patient Education Diabetes ReportDocument76 pagesStructured Patient Education Diabetes ReportPatrick Commettant100% (1)
- Harm Reduction Program April 2013Document33 pagesHarm Reduction Program April 2013PUSAT LATIHAN AADKNo ratings yet
- Septic AbortionDocument15 pagesSeptic Abortionapi-3705046No ratings yet
- Early Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsFrom EverandEarly Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsNo ratings yet
- Final Novo NordiskDocument5 pagesFinal Novo Nordiskusamafunky100% (1)
- National ART Clinical Guideline 2023 - 04 - 28 SignedDocument44 pagesNational ART Clinical Guideline 2023 - 04 - 28 SignedZimkita Zintle MakeleniNo ratings yet
- Sri Lanka-ADB Partnership: 1966-2016Document156 pagesSri Lanka-ADB Partnership: 1966-2016Asian Development Bank100% (2)
- Integrated Management of Childhood Illnesses in NigeriaDocument32 pagesIntegrated Management of Childhood Illnesses in NigeriaIfedigbo-Ejidike Nwamaka100% (8)
- Antimicrobial StewardshipDocument40 pagesAntimicrobial StewardshipChestnutNo ratings yet
- Ibrahim Kalin - Knowledge in Later Islamic Philosophy - Mulla Sadra On Existence, Intellect, and Intuition (2010) PDFDocument338 pagesIbrahim Kalin - Knowledge in Later Islamic Philosophy - Mulla Sadra On Existence, Intellect, and Intuition (2010) PDFBarış Devrim Uzun100% (1)
- 2014 - ACT Consortium - EARN HandoutDocument5 pages2014 - ACT Consortium - EARN HandoutnomdeplumNo ratings yet
- National Leprosy Eradication Program (Nlep: Dr. Kanupriya ChaturvediDocument24 pagesNational Leprosy Eradication Program (Nlep: Dr. Kanupriya ChaturvediLavendra KunwarNo ratings yet
- Hope in The Pipeline: New Drugs (Bedaquiline/Sirturo, Delamanid/Deltyba)Document24 pagesHope in The Pipeline: New Drugs (Bedaquiline/Sirturo, Delamanid/Deltyba)National Press FoundationNo ratings yet
- Treatment of African Children With Severe Malaria - Towards Evidence-Informed Clinical Practice Using GradeDocument10 pagesTreatment of African Children With Severe Malaria - Towards Evidence-Informed Clinical Practice Using GradeFrc 'Hario' FanachaNo ratings yet
- Doh ProgramsDocument14 pagesDoh ProgramsSweetyfe GabatanNo ratings yet
- IMCI UpdatesDocument5 pagesIMCI UpdatesJaypee Ravina100% (2)
- Effect of Postpartum Family Planning Counseling On Adoption & Continuation of Modern Contraceptive MethodsDocument14 pagesEffect of Postpartum Family Planning Counseling On Adoption & Continuation of Modern Contraceptive MethodsMaternal and Child Survival Program (MCSP)No ratings yet
- CCM: Community: Sumberdaya Dan Kebijakan KomunitasDocument53 pagesCCM: Community: Sumberdaya Dan Kebijakan KomunitasAlvinNo ratings yet
- Community Case Management: BY:Nathifa Abdi H31/34946/2013 and Busaidy Swafiya H31/2369/2012Document37 pagesCommunity Case Management: BY:Nathifa Abdi H31/34946/2013 and Busaidy Swafiya H31/2369/2012okwadha simionNo ratings yet
- Management of Infection Guidance For Primary Care For Consultation and Local Adaptation - July 2015Document66 pagesManagement of Infection Guidance For Primary Care For Consultation and Local Adaptation - July 2015neleatucicovshiiNo ratings yet
- Wepik Optimizing Covid 19 Care Strategies 20240401084945ckV9Document8 pagesWepik Optimizing Covid 19 Care Strategies 20240401084945ckV9janetNo ratings yet
- NTEP or RNTCP (Community Health Nursing)Document37 pagesNTEP or RNTCP (Community Health Nursing)Ankita ShaluNo ratings yet
- Family Planning CouncellingDocument6 pagesFamily Planning CouncellingNyakie MotlalaneNo ratings yet
- IETP Assessment Learning Outcome Mapping v2 FINALDocument19 pagesIETP Assessment Learning Outcome Mapping v2 FINALManar SiddiqNo ratings yet
- 2017 - 2022 Philippine Strategic TB Elimination Plan: Phase 1 (Philstep1)Document25 pages2017 - 2022 Philippine Strategic TB Elimination Plan: Phase 1 (Philstep1)Jon ObilloNo ratings yet
- Strengthening The Capacity of Healthcare Providers To Administer Intermittent Preventive Therapy For Malaria in Pregnancy in Nigeria Using A Quality Improvement StrategyDocument13 pagesStrengthening The Capacity of Healthcare Providers To Administer Intermittent Preventive Therapy For Malaria in Pregnancy in Nigeria Using A Quality Improvement StrategyEjemai EboreimeNo ratings yet
- Research Presentation by Batch 32Document29 pagesResearch Presentation by Batch 32Usama QamarNo ratings yet
- Continous Quality Improvement Made PossibleDocument21 pagesContinous Quality Improvement Made Possiblejohn488No ratings yet
- Cervical and Breast Cancer: Community Health Service and Community Mobilization DevelopmentDocument16 pagesCervical and Breast Cancer: Community Health Service and Community Mobilization DevelopmentIndonesian Journal of CancerNo ratings yet
- Jurnal 1Document12 pagesJurnal 1Riafinola IfanisariNo ratings yet
- National Minimum Prevention MPPI GuideDocument20 pagesNational Minimum Prevention MPPI GuideEmmanuel Umo EffiongNo ratings yet
- Deprescribing Proton Pump InhibitorsDocument11 pagesDeprescribing Proton Pump InhibitorsAngela CerlatNo ratings yet
- Algoritmo IctericiaDocument18 pagesAlgoritmo IctericiaDiego RodriguezNo ratings yet
- Doh Health Programs 1Document139 pagesDoh Health Programs 1Eric VeranoNo ratings yet
- FIGO HIP For Website 21 Feb 17Document46 pagesFIGO HIP For Website 21 Feb 17Bob IrsanNo ratings yet
- Indian J Community MedDocument5 pagesIndian J Community MedImam Hakim SuryonoNo ratings yet
- National Health Programmes On Communicable and Non Communicable Diseases - ANAND MLHPDocument37 pagesNational Health Programmes On Communicable and Non Communicable Diseases - ANAND MLHPAnand gowdaNo ratings yet
- ISQua Webinar - Nick Sevdalis - September 2017Document39 pagesISQua Webinar - Nick Sevdalis - September 2017utari dewiNo ratings yet
- Prevention and Health Promotion 2023SSDocument39 pagesPrevention and Health Promotion 2023SSzeynepNo ratings yet
- Assignment For National T.B ProgramDocument14 pagesAssignment For National T.B Programhaitham thabetNo ratings yet
- Cyprien Nioble, Jhpiego-Cote Divoire, IAS2012 Poster, MNH Quality ImprovementDocument1 pageCyprien Nioble, Jhpiego-Cote Divoire, IAS2012 Poster, MNH Quality ImprovementJhpiegoNo ratings yet
- Technical PackageDocument112 pagesTechnical Packagecristi.leytonNo ratings yet
- Adult Primary Care GuideDocument156 pagesAdult Primary Care GuideKatieNo ratings yet
- Background/Situational AnalysisDocument7 pagesBackground/Situational AnalysisSimon DzokotoNo ratings yet
- 3 Medication AdherenceDocument19 pages3 Medication AdherenceKrishelle Anne ObispoNo ratings yet
- ProcessDocument2 pagesProcessaleena.docsNo ratings yet
- Zinc DeficiencyDocument24 pagesZinc DeficiencyElita Maritan SNo ratings yet
- Doh Programs ShortcutDocument26 pagesDoh Programs ShortcutSai BondadNo ratings yet
- Revised National Tuberculosis Control ProgramDocument2 pagesRevised National Tuberculosis Control ProgramBMO BarsarNo ratings yet
- Alben Daz OleDocument5 pagesAlben Daz OleTariqNo ratings yet
- RCH - Reproductive and Child Health Part 2Document32 pagesRCH - Reproductive and Child Health Part 2Dr. Rakshit SolankiNo ratings yet
- LegalaspectsDocument38 pagesLegalaspectswiss gaderNo ratings yet
- Outline of Presentation: Evolving Malaria Control Strategies in India. NVBDCPDocument33 pagesOutline of Presentation: Evolving Malaria Control Strategies in India. NVBDCPritikaritikaNo ratings yet
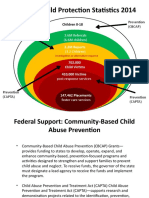
- National Child Protection Statistics 2014: Prevention (Cbcap) Prevention (Capta)Document14 pagesNational Child Protection Statistics 2014: Prevention (Cbcap) Prevention (Capta)MarryRose Dela Torre FerrancoNo ratings yet
- Health Programs in India - RNTCPDocument28 pagesHealth Programs in India - RNTCPAkash Mittal100% (1)
- PRESENTATION: Asia Pacific's Health Trends-Obesity, NCDs and ADB's Operational Plan For Health 2015-2020Document40 pagesPRESENTATION: Asia Pacific's Health Trends-Obesity, NCDs and ADB's Operational Plan For Health 2015-2020ADB Health Sector GroupNo ratings yet
- Evaluating The NHS Diabetes Prevention Programme (NHS DPP) : The DIPLOMA Research Programme (Diabetes Prevention - Long Term Multimethod Assessment) ProtocolDocument27 pagesEvaluating The NHS Diabetes Prevention Programme (NHS DPP) : The DIPLOMA Research Programme (Diabetes Prevention - Long Term Multimethod Assessment) ProtocolVu BuiNo ratings yet
- 3089 File E3 OliverosDocument22 pages3089 File E3 OliverosDanna Michelle Kay FlojoNo ratings yet
- 2011 National Policy On Diagnosis and Treatment of MalariaDocument34 pages2011 National Policy On Diagnosis and Treatment of MalarianoblefxNo ratings yet
- 2.BPAL Presentation - WHODocument20 pages2.BPAL Presentation - WHOHamka HamkaNo ratings yet
- Detrusor InstabilityDocument7 pagesDetrusor Instabilityapi-3705046No ratings yet
- Ovarian TumoursDocument17 pagesOvarian Tumoursapi-3705046100% (3)
- Current Management of LabourDocument48 pagesCurrent Management of Labourapi-3705046100% (4)
- Vulvar MalignancyDocument21 pagesVulvar Malignancyapi-3705046No ratings yet
- Cervical Incompetence 1Document5 pagesCervical Incompetence 1api-3705046100% (1)
- Weight Gain in PregnancyDocument18 pagesWeight Gain in Pregnancyapi-3705046No ratings yet
- HODocument14 pagesHOapi-3705046No ratings yet
- VVF Clinical Presentation 1Document24 pagesVVF Clinical Presentation 1api-370504683% (6)
- The Incompetent Cervix 1Document10 pagesThe Incompetent Cervix 1api-3705046100% (1)
- Vaginal Birth After Caesarean Section (Vbac)Document16 pagesVaginal Birth After Caesarean Section (Vbac)api-370504650% (2)
- Vesico Vaginal FistulaDocument6 pagesVesico Vaginal Fistulaapi-3705046No ratings yet
- Thyroid Diseases in PregnancyDocument18 pagesThyroid Diseases in Pregnancyapi-3705046100% (3)
- Unstable LieDocument7 pagesUnstable Lieapi-370504667% (3)
- Uterine FibroidsDocument11 pagesUterine Fibroidsapi-3705046No ratings yet
- Roll Back MalariaDocument2 pagesRoll Back Malariaapi-3705046No ratings yet
- Uterovaginal ProlapseDocument16 pagesUterovaginal Prolapseapi-3705046100% (1)
- The Incompetent Cervix 2Document30 pagesThe Incompetent Cervix 2api-3705046100% (3)
- Renal Disease in PregDocument22 pagesRenal Disease in Pregapi-3705046100% (1)
- Reprodctive HealthDocument4 pagesReprodctive Healthapi-3705046No ratings yet
- Preeclampsia and EclampsiaDocument23 pagesPreeclampsia and Eclampsiaapi-3705046100% (6)
- PubertyDocument7 pagesPubertyapi-3705046No ratings yet
- Preterm Rupture of Foetal MembranesDocument24 pagesPreterm Rupture of Foetal Membranesapi-3705046No ratings yet
- Feedback For Question 1-MIDTERM 2 AFM 451Document2 pagesFeedback For Question 1-MIDTERM 2 AFM 451jason fNo ratings yet
- Entity Relationship Diagram: TBL - Students TBL - ProgramsDocument1 pageEntity Relationship Diagram: TBL - Students TBL - ProgramsEun Chae KimNo ratings yet
- 17. ĐỀ SỐ 17 HSG ANH 9 HUYỆNDocument9 pages17. ĐỀ SỐ 17 HSG ANH 9 HUYỆNHồng Hoàn NguyễnNo ratings yet
- Discourse Analysis: Understanding How We Understand.: Ey WordDocument7 pagesDiscourse Analysis: Understanding How We Understand.: Ey WordTommy NickelsonNo ratings yet
- PTE Self Study - Lfib v3.0Document57 pagesPTE Self Study - Lfib v3.0Jewel AhmedNo ratings yet
- Forecasting The Return Volatility of The Exchange RateDocument53 pagesForecasting The Return Volatility of The Exchange RateProdan IoanaNo ratings yet
- Cambridge AS Business SyllabusDocument2 pagesCambridge AS Business SyllabusEnox ChangNo ratings yet
- Jurnal Internasional Tentang ScabiesDocument9 pagesJurnal Internasional Tentang ScabiesGalyNo ratings yet
- Structural Dynamics: 10/11/2017 Dynamic Analysis 1Document110 pagesStructural Dynamics: 10/11/2017 Dynamic Analysis 1Mohammed Essam ShatnawiNo ratings yet
- BS 8901 SEG Press ReleaseDocument3 pagesBS 8901 SEG Press Releasetjsunder449No ratings yet
- DonnetDocument12 pagesDonnetAsia SzmyłaNo ratings yet
- Arulanandan Soil Structure PDFDocument251 pagesArulanandan Soil Structure PDFchongptNo ratings yet
- Nina Harris Mira Soskis Thalia Ehrenpreis Stella Martin and Lily Edwards - Popper Lab Write UpDocument4 pagesNina Harris Mira Soskis Thalia Ehrenpreis Stella Martin and Lily Edwards - Popper Lab Write Upapi-648007364No ratings yet
- Waqas Ahmed C.VDocument2 pagesWaqas Ahmed C.VWAQAS AHMEDNo ratings yet
- 9-12 Lesson PlanDocument3 pages9-12 Lesson Planapi-364700795No ratings yet
- استخدام الشبكة الإدارية في السلوك القيادي بحث محكمDocument22 pagesاستخدام الشبكة الإدارية في السلوك القيادي بحث محكمsalm yasmenNo ratings yet
- Eng 1: Communication Arts: Talisay City CollegeDocument14 pagesEng 1: Communication Arts: Talisay City CollegeDennis SocuanoNo ratings yet
- Generative Drafting (ISO) : CATIA TrainingDocument148 pagesGenerative Drafting (ISO) : CATIA TrainingAnonymous 38RNNHWyNo ratings yet
- Application For Bir Number: Board of Inland RevenueDocument2 pagesApplication For Bir Number: Board of Inland Revenuedinesh007No ratings yet
- Derrida, Declarations of Independence PDFDocument7 pagesDerrida, Declarations of Independence PDFMichael Litwack100% (1)
- NSF Science and Engineering Indicators 2014Document600 pagesNSF Science and Engineering Indicators 2014Adrian ArizmendiNo ratings yet