You might also like
- Substance Abuse Case PresentationDocument10 pagesSubstance Abuse Case Presentationapi-3703352100% (2)
- Aortic AneurysmDocument61 pagesAortic AneurysmSurya Budikusuma64% (11)
- Manitoba OSCE Book PDFDocument267 pagesManitoba OSCE Book PDFVlad75% (4)
- Obstetric and Gynecology ExamDocument14 pagesObstetric and Gynecology Examapi-3703352No ratings yet
- Raza2004 PDFDocument12 pagesRaza2004 PDFIvana RuseskaNo ratings yet
- Moriyama Dan Takahashi, 2016.Document12 pagesMoriyama Dan Takahashi, 2016.Jeje MystearicaNo ratings yet
- Efficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsDocument13 pagesEfficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsAdityasekar WangiNo ratings yet
- Prevalence of Dyslipidemia and Other Cardiovascular Risk Factors (Hypertension and Diabetes) in Medical ProfessionalsDocument5 pagesPrevalence of Dyslipidemia and Other Cardiovascular Risk Factors (Hypertension and Diabetes) in Medical ProfessionalsTirth NathwaniNo ratings yet
- Remnant CholesterolDocument3 pagesRemnant CholesterolExia WuNo ratings yet
- Narsum 1 Tatalaksana DislipidemiaDocument32 pagesNarsum 1 Tatalaksana DislipidemiabimaNo ratings yet
- Cardio Metabolic Risk in DiabetesDocument29 pagesCardio Metabolic Risk in DiabetesoctoindradjajaNo ratings yet
- Gender Difference in Coronary Events in Relation To Risk Factors in Japanese Hypercholesterolemic Patients Treated With Low-Dose SimvastatinDocument5 pagesGender Difference in Coronary Events in Relation To Risk Factors in Japanese Hypercholesterolemic Patients Treated With Low-Dose SimvastatinasfwegereNo ratings yet
- Lipoprotein Paper Academia ZaragedDocument29 pagesLipoprotein Paper Academia Zaragedpawovem755No ratings yet
- Triglyceride Profile in Dyslipidaemia of Type 2 Diabetes MellitusDocument4 pagesTriglyceride Profile in Dyslipidaemia of Type 2 Diabetes MellitusTanveerNo ratings yet
- Clinical Science High Ratio of Triglycerides To Hdl-Cholesterol Predicts Extensive Coronary DiseaseDocument6 pagesClinical Science High Ratio of Triglycerides To Hdl-Cholesterol Predicts Extensive Coronary DiseaseMarj MendezNo ratings yet
- Cho Paradigm For Reduction of ASCVDDocument17 pagesCho Paradigm For Reduction of ASCVDBubu ToNo ratings yet
- The Effects of Menopause On The Serum Lipid Profile of Normal Females of South East Nigeria J. C. Igweh, I. U. Nwagha, J. M. OkaroDocument6 pagesThe Effects of Menopause On The Serum Lipid Profile of Normal Females of South East Nigeria J. C. Igweh, I. U. Nwagha, J. M. OkaroutarinuNo ratings yet
- Coronary Heart Disease Risk Factors Among UniversiDocument6 pagesCoronary Heart Disease Risk Factors Among UniversiMuhammad Irfan JamilNo ratings yet
- Supersize Teens - The Metabolic Syndrome.Document23 pagesSupersize Teens - The Metabolic Syndrome.Milon MitraNo ratings yet
- Dyslipidemia Management in Women and Men: Exploring Potential Gender DifferencesDocument7 pagesDyslipidemia Management in Women and Men: Exploring Potential Gender DifferencesAmelie AnsonNo ratings yet
- Association Between Baseline LDL-C Level and TotalDocument14 pagesAssociation Between Baseline LDL-C Level and TotalMr. LNo ratings yet
- A Comparison of Statin Therapies in Hypercholesterolemia in Women: A Subgroup Analysis of The STELLAR StudyDocument7 pagesA Comparison of Statin Therapies in Hypercholesterolemia in Women: A Subgroup Analysis of The STELLAR StudyFa'iq Hanif MubarokNo ratings yet
- LDL InggDocument7 pagesLDL InggDuti AprilniNo ratings yet
- Methods For Measuremnent of LDL CholesterolDocument19 pagesMethods For Measuremnent of LDL Cholesterolmaheren tubeNo ratings yet
- Lipid Profile and Antihypertensive Drugs: Al-Kindy Col Med J 2009 Vol .5 (1) P:1-4Document4 pagesLipid Profile and Antihypertensive Drugs: Al-Kindy Col Med J 2009 Vol .5 (1) P:1-4Septi Fadhilah SPNo ratings yet
- Influence of Triglycerides On Other Plasma Lipids in Middle-Aged Men Intended For Hypolipidaemic TreatmentDocument6 pagesInfluence of Triglycerides On Other Plasma Lipids in Middle-Aged Men Intended For Hypolipidaemic TreatmentPatrisia HallaNo ratings yet
- Dyslipidemia Management in Diabetic Patient: Putu Moda Arsana FKUB, Malang, 2016Document31 pagesDyslipidemia Management in Diabetic Patient: Putu Moda Arsana FKUB, Malang, 2016aprinaaaNo ratings yet
- Cardiometabolic Syndrome: & DR Dhafir A. MahmoodDocument62 pagesCardiometabolic Syndrome: & DR Dhafir A. MahmoodJacob AlphaNo ratings yet
- RosuvastatinDocument62 pagesRosuvastatinEileen del RosarioNo ratings yet
- JNC VIII Hypertension SaudiDocument47 pagesJNC VIII Hypertension SaudiDavid Chandra EriksonNo ratings yet
- Recommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (AdaptedDocument8 pagesRecommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (Adaptedعزالدين الطيارNo ratings yet
- Dislipidemia ACP 2017Document16 pagesDislipidemia ACP 2017José Luis PradoNo ratings yet
- HDL Muy Alto 2019Document10 pagesHDL Muy Alto 2019Luis C Ribon VNo ratings yet
- SDL DL BrochureDocument2 pagesSDL DL BrochureNanda Nabilah UbayNo ratings yet
- Triglyceride-to-HDL Cholesterol Ratio in The Dyslipidemic Classification of Type 2 DiabetesDocument3 pagesTriglyceride-to-HDL Cholesterol Ratio in The Dyslipidemic Classification of Type 2 DiabetesfitrianNo ratings yet
- New England Journal Medicine: The ofDocument13 pagesNew England Journal Medicine: The ofStefania CristinaNo ratings yet
- New Treatments of Hypercholesterolemia: Jason A. Logan Family Medicine Clerkship Presentation 4/27/01Document41 pagesNew Treatments of Hypercholesterolemia: Jason A. Logan Family Medicine Clerkship Presentation 4/27/01Saad MotawéaNo ratings yet
- Jurnal CardioDocument7 pagesJurnal CardioJicko Street HooligansNo ratings yet
- 8E - Lipid Sirt Study JANA 2010Document6 pages8E - Lipid Sirt Study JANA 2010alonso martinNo ratings yet
- Management of HyperlipidemiaDocument34 pagesManagement of HyperlipidemiaCarleta StanNo ratings yet
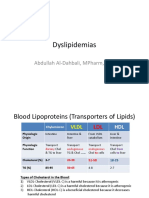
- Dyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDDocument15 pagesDyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDعزالدين الطيارNo ratings yet
- 2018 Dislipidemia-RevisaDocument16 pages2018 Dislipidemia-RevisaLuminita HutanuNo ratings yet
- ProjectDocument32 pagesProjectNithya sudevNo ratings yet
- Ezetimibe - A Novel Add On Treatment Strategy To Achieve Targeted LDL in Patients With Uncontrolled LDL Levels On High Dose Statin AloneDocument9 pagesEzetimibe - A Novel Add On Treatment Strategy To Achieve Targeted LDL in Patients With Uncontrolled LDL Levels On High Dose Statin AloneEditor ERWEJNo ratings yet
- Remnant Cholesterol As A Causal Risk Factor For Ischemic Heart DiseaseDocument10 pagesRemnant Cholesterol As A Causal Risk Factor For Ischemic Heart DiseaseIonuț CozmaNo ratings yet
- Jhs v3 Id1044 PDFDocument4 pagesJhs v3 Id1044 PDFUrsheila HaekmatiarNo ratings yet
- Achievement of Target LDL-C in Type 2 DM Patients in Saudi ArabiaDocument4 pagesAchievement of Target LDL-C in Type 2 DM Patients in Saudi ArabiaIJAR JOURNALNo ratings yet
- The Association Between The Triglyceride To High-Density Lipoprotein Cholesterol Ratio and Low-Density Lipoprotein SubclassesDocument9 pagesThe Association Between The Triglyceride To High-Density Lipoprotein Cholesterol Ratio and Low-Density Lipoprotein SubclassesHendro GunawanNo ratings yet
- Optimal Low-Density Lipoprotein Is 50 To 70 Mg:Dl... 1Document1 pageOptimal Low-Density Lipoprotein Is 50 To 70 Mg:Dl... 1Odessa FileNo ratings yet
- Atherosclerosis, Dyslipidaemia and Diabetes SlidesDocument83 pagesAtherosclerosis, Dyslipidaemia and Diabetes SlidesTatiana GobjilăNo ratings yet
- DyslipidemiaManagement Continuum 2011Document13 pagesDyslipidemiaManagement Continuum 2011Zuleika DöObsönNo ratings yet
- Diagnosis and Managment of Peripheral Artery Disease Gore Updated DR KrolickDocument88 pagesDiagnosis and Managment of Peripheral Artery Disease Gore Updated DR KrolickLeo OoNo ratings yet
- Diagnosis and Managment of Peripheral Artery Disease Gore Updated DR KrolickDocument88 pagesDiagnosis and Managment of Peripheral Artery Disease Gore Updated DR KrolickLeo OoNo ratings yet
- Journal of Diabetes and Its ComplicationsDocument6 pagesJournal of Diabetes and Its ComplicationsNadia Rezky ElizaNo ratings yet
- Pharmacology & Therapeutics: Anette Varbo, Marianne Benn, Børge G. NordestgaardDocument10 pagesPharmacology & Therapeutics: Anette Varbo, Marianne Benn, Børge G. NordestgaardIonuț CozmaNo ratings yet
- Role of Rosuvastatin in The Treatment of DyslipidemiaDocument16 pagesRole of Rosuvastatin in The Treatment of DyslipidemiaabcdefNo ratings yet
- 1 s2.0 S0735109722064920 MainDocument2 pages1 s2.0 S0735109722064920 MainRapee JarungsirawatNo ratings yet
- Metabolic Syndrome, Diabetes, and Cardiovascular Disease: Implications For Preventive CardiologyDocument36 pagesMetabolic Syndrome, Diabetes, and Cardiovascular Disease: Implications For Preventive CardiologyAlvianridersNo ratings yet
- Correlation of Dyslipidemia and Type 2 Diabetes Mellitus Amongst The People of Vidarbha Region of IndiaDocument6 pagesCorrelation of Dyslipidemia and Type 2 Diabetes Mellitus Amongst The People of Vidarbha Region of IndiaKiki FatmawatyNo ratings yet
- The Relationship Between Hba1C and Lipid Profile in Type 2 Diabetic Saudi PatientsDocument6 pagesThe Relationship Between Hba1C and Lipid Profile in Type 2 Diabetic Saudi PatientsnaxxxNo ratings yet
- JurnalBiokim PDFDocument3 pagesJurnalBiokim PDFRini LiliNo ratings yet
- 1 s2.0 S000291491830612X MainDocument1 page1 s2.0 S000291491830612X MainRiYaan Ali AliNo ratings yet
- 2008 Article BF02867401Document8 pages2008 Article BF02867401fachrurNo ratings yet
- 18 Psychosexual DisorderDocument15 pages18 Psychosexual Disorderapi-3703352No ratings yet
- Destigmatization of Psychiatric PatientsDocument15 pagesDestigmatization of Psychiatric Patientsapi-3703352No ratings yet
- Psychiatry ExamDocument4 pagesPsychiatry Examapi-3703352No ratings yet
- Suicide and DSHDocument6 pagesSuicide and DSHapi-3703352No ratings yet
- Schizophrenia: at The End of The Lecture You Should Be Able ToDocument18 pagesSchizophrenia: at The End of The Lecture You Should Be Able Toapi-3703352No ratings yet
- Neurotic, Stress-Related and Somatoform DisDocument17 pagesNeurotic, Stress-Related and Somatoform Disapi-3703352No ratings yet
- Delusional DisorderDocument3 pagesDelusional Disorderapi-3703352No ratings yet
- Insomnia: Assessment & ManagementDocument5 pagesInsomnia: Assessment & Managementapi-3703352No ratings yet
- Liaison PsychiatryDocument5 pagesLiaison Psychiatryapi-3703352No ratings yet
- 11-Evaluation of Fetal Well-Being Sept01Document59 pages11-Evaluation of Fetal Well-Being Sept01api-3703352100% (1)
- PsychopharmacologyDocument50 pagesPsychopharmacologyapi-3703352No ratings yet
- Alcohol Misuse: Dr. Adel Alzayed Kuwait University - Medical CollegeDocument28 pagesAlcohol Misuse: Dr. Adel Alzayed Kuwait University - Medical Collegeapi-3703352No ratings yet
- Intrauterine Growth Restriction: Dr. Majed Alshammari, FRSCSDocument72 pagesIntrauterine Growth Restriction: Dr. Majed Alshammari, FRSCSapi-3703352No ratings yet
- 13-Pregnancy & DMDocument50 pages13-Pregnancy & DMapi-3703352No ratings yet
- 11-Evaluation of Fetal Well-Being Nov2000Document7 pages11-Evaluation of Fetal Well-Being Nov2000api-3703352No ratings yet
- DR - Jassim Al-Hijji: Adan HospitalDocument79 pagesDR - Jassim Al-Hijji: Adan Hospitalapi-3703352No ratings yet
- 16-Genital ProlapseDocument37 pages16-Genital Prolapseapi-3703352No ratings yet
- Adaptive Changes in Pregnancy: DR - Nandakumaran MoorkathDocument82 pagesAdaptive Changes in Pregnancy: DR - Nandakumaran Moorkathapi-3703352No ratings yet
- 4-Drugs in Obs & GyneDocument52 pages4-Drugs in Obs & Gyneapi-37033520% (2)
- Infertility, Investigation and Management: Dr. Raedah Al-FadhliDocument64 pagesInfertility, Investigation and Management: Dr. Raedah Al-Fadhliapi-3703352No ratings yet
- 6th y Abdomen X-RayDocument68 pages6th y Abdomen X-Rayapi-3703352No ratings yet
- Vital Sign #1: Body TemperatureDocument5 pagesVital Sign #1: Body TemperaturePrimelift Safety Resources LimitedNo ratings yet
- How To Analyze EkgsDocument40 pagesHow To Analyze EkgsJosh WeisNo ratings yet
- A18 BODY FLUIDS in Human BodyDocument1 pageA18 BODY FLUIDS in Human Bodyservoculus machatteNo ratings yet
- Oet Writing Tasks Final-12-14Document3 pagesOet Writing Tasks Final-12-14MK Exam SectionNo ratings yet
- Allen: (Conceptual Questions)Document24 pagesAllen: (Conceptual Questions)Sachin Kumar GautamNo ratings yet
- Chapter 13: The Heart and Heart DiseaseDocument3 pagesChapter 13: The Heart and Heart Diseasetrbrown2011No ratings yet
- Quick Reference Guide: R SeriesDocument12 pagesQuick Reference Guide: R SeriesA. A.G.No ratings yet
- Wiggers Diagram SlidesDocument15 pagesWiggers Diagram SlidesKuro ShiroNo ratings yet
- Chapter 13 Cardiovascular ResponsesDocument32 pagesChapter 13 Cardiovascular ResponsesMARIA FERNANDA RONDONNo ratings yet
- Raport StimulatorDocument88 pagesRaport StimulatorEghet SilviuNo ratings yet
- Cardio 21 Group Assignment Review - NPTE Final FrontierDocument19 pagesCardio 21 Group Assignment Review - NPTE Final FrontierNPTE بالعربيNo ratings yet
- ACLS Saroa Et AlDocument17 pagesACLS Saroa Et AlMarc Andreo MalalaNo ratings yet
- Electrocardiografia BasicaDocument49 pagesElectrocardiografia BasicaENRIQUEVERSAGNo ratings yet
- Myocardial Infraction ImprovedDocument14 pagesMyocardial Infraction Improvedvikram yadavNo ratings yet
- Electrocardiogram Nursing ResponsibilitiesDocument28 pagesElectrocardiogram Nursing ResponsibilitiesKristine Jade Rojas100% (1)
- Anph121lb CardiovascularDocument28 pagesAnph121lb CardiovascularDANIELA PEREZNo ratings yet
- Congestive Heart FailureDocument29 pagesCongestive Heart FailureAbby Ang100% (3)
- Ezx 314Document29 pagesEzx 314Adventa 91No ratings yet
- Omron RX 1 Users Manual 332474Document9 pagesOmron RX 1 Users Manual 332474kuntakinte22No ratings yet
- Physiology Mid Q Part 3 VIPDocument16 pagesPhysiology Mid Q Part 3 VIPDanah AlhusainiNo ratings yet
- MURMURDocument21 pagesMURMURtoyyibNo ratings yet
- The Human Circulatory System by TariqDocument84 pagesThe Human Circulatory System by TariqMuhammad Tariq KhanNo ratings yet
- Pathophysiology Tia VS CvaDocument6 pagesPathophysiology Tia VS CvaRobby Nur Zam ZamNo ratings yet
- MODULE 1.1 and 1.2 SOFTDocument5 pagesMODULE 1.1 and 1.2 SOFTJason SebastianNo ratings yet
- 452l Simulation 6 Pre SimulationDocument9 pages452l Simulation 6 Pre Simulationapi-307439819No ratings yet
- 1 Tolerancia Al Esfuerzo MyersDocument9 pages1 Tolerancia Al Esfuerzo MyersAMALIANo ratings yet
- ECHO CensusDocument9 pagesECHO CensusReda SoNo ratings yet
- Tachycardia With A Pulse Algorithm: Assess Appropriateness For Clinical ConditionDocument1 pageTachycardia With A Pulse Algorithm: Assess Appropriateness For Clinical ConditionDendy Frannuzul RamadhanNo ratings yet