You might also like
- Cardiac DisordersDocument15 pagesCardiac Disordersgold_enriquez100% (3)
- Acls Study GuideDocument24 pagesAcls Study GuideMohammad Gita100% (17)
- ACLS Simplify AlgorithmDocument6 pagesACLS Simplify AlgorithmKristine Monforte Coma UritaNo ratings yet
- Cardiac ArrythmiasDocument63 pagesCardiac ArrythmiasSankara SubramanianNo ratings yet
- Sample ChartingDocument4 pagesSample Chartinggreen_archer100% (1)
- Family Medicine EORDocument159 pagesFamily Medicine EORAndrew BowmanNo ratings yet
- 12 Lead ECG and STEMI BasicsDocument91 pages12 Lead ECG and STEMI BasicsCaroline TaylorNo ratings yet
- Basicecginterpretationpracticetestv1 AshxDocument7 pagesBasicecginterpretationpracticetestv1 AshxEdward ZiyachechaNo ratings yet
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!From EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!No ratings yet
- Google Doc - Mark K NCLEX Study GuideDocument62 pagesGoogle Doc - Mark K NCLEX Study Guideezinne obinna-umaNo ratings yet
- Electrocardiography (Ecg) : Presented By: Fahad I. HussienDocument102 pagesElectrocardiography (Ecg) : Presented By: Fahad I. HussienMustafa A. DawoodNo ratings yet
- Chapter - 036 Arrhythmias ClassDocument129 pagesChapter - 036 Arrhythmias ClassWisdomIsMiseryNo ratings yet
- Ekg Made EasyDocument7 pagesEkg Made Easystring44100% (3)
- Arrhythmias: Sing Khien Tiong Gpst1Document34 pagesArrhythmias: Sing Khien Tiong Gpst1preethi preethaNo ratings yet
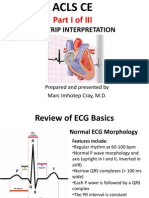
- ACLS CE-Part I of III - ECG Strip Interpretation W Case Scenarios SupplementalDocument80 pagesACLS CE-Part I of III - ECG Strip Interpretation W Case Scenarios SupplementalMarc Imhotep Cray, M.D.100% (2)
- CardionotesDocument5 pagesCardionotesNichole Coletta100% (1)
- ACLS Algorithms Adult 2010 Revised May 31 2011Document12 pagesACLS Algorithms Adult 2010 Revised May 31 2011arturschander3614No ratings yet
- ACLS Appendix 3Document32 pagesACLS Appendix 3tostc100% (1)
- Internal Medicine NotesDocument26 pagesInternal Medicine NotesPierce ArthurNo ratings yet
- Basic Arrythmias: Prof. Maximin A. Pomperada, RN, MNDocument70 pagesBasic Arrythmias: Prof. Maximin A. Pomperada, RN, MNRellie CastroNo ratings yet
- Basic Arrythmia AnalysisDocument60 pagesBasic Arrythmia AnalysisZakky KurniawanNo ratings yet
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- Quiz Let Mark YellowDocument32 pagesQuiz Let Mark Yellowharlb95% (20)
- Torsade De Pointes, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandTorsade De Pointes, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- CPR SeminarDocument76 pagesCPR SeminarAmy Lalringhluani Chhakchhuak100% (3)
- ACLS MedicationsDocument31 pagesACLS MedicationscmirceaNo ratings yet
- Megacode Simulator 1Document10 pagesMegacode Simulator 1srimatsimhasaneshwarNo ratings yet
- Cardiac Emergencies Cne DelhiDocument109 pagesCardiac Emergencies Cne DelhiManisha Thakur100% (1)
- Roberto Santilli - Electrocardiography of The Dog and Cat - Diagnosis of Arrhythmias-Edra (2018)Document348 pagesRoberto Santilli - Electrocardiography of The Dog and Cat - Diagnosis of Arrhythmias-Edra (2018)Juan DuasoNo ratings yet
- Atrial FlutterDocument16 pagesAtrial Flutterapi-527603714100% (1)
- Standford Emergency Manual Interactive 2021Document60 pagesStandford Emergency Manual Interactive 2021reinaldo valdes iznagaNo ratings yet
- Aritmia LetalDocument49 pagesAritmia LetalfebriyakNo ratings yet
- Syncope: UCI Internal Medicine Core Curriculum - Mini LectureDocument15 pagesSyncope: UCI Internal Medicine Core Curriculum - Mini LecturechandanNo ratings yet
- Pathophysiology of ArrhythmiasDocument15 pagesPathophysiology of ArrhythmiasJonathan MontecilloNo ratings yet
- Cerebrovascular Accidents: Stroke Versus TIADocument19 pagesCerebrovascular Accidents: Stroke Versus TIASagar ShahNo ratings yet
- Electrocardiogram: Electrocardiogram EKG Heart Heart's Electrical Activity DiagnosisDocument38 pagesElectrocardiogram: Electrocardiogram EKG Heart Heart's Electrical Activity DiagnosislorhenzsoNo ratings yet
- Electro Cardiograph yDocument94 pagesElectro Cardiograph ykajonasfoodproductsNo ratings yet
- Cardiac ArrestDocument40 pagesCardiac ArrestApriliani Nur Puspita SariNo ratings yet
- Perfusion. Dysrhythmias - Pacemaker.aicdDocument41 pagesPerfusion. Dysrhythmias - Pacemaker.aicdMichael S. PetryNo ratings yet
- Pradheep ProjectDocument20 pagesPradheep ProjectHaribabuBabuNo ratings yet
- Advanced Cardiac Life Support (ACLS)Document17 pagesAdvanced Cardiac Life Support (ACLS)Siti Rahima HarahapNo ratings yet
- Aritmia LetalDocument53 pagesAritmia LetalMetta SariNo ratings yet
- Cardiac Arrhythmia in Children PDFDocument50 pagesCardiac Arrhythmia in Children PDFNorhafizah AhmadNo ratings yet
- Spring 2014 NewsletterDocument5 pagesSpring 2014 Newsletterapi-236445988No ratings yet
- Management of Cardiac ArrestDocument40 pagesManagement of Cardiac ArrestMark Francis NaniaNo ratings yet
- A Patient With PalpitationDocument43 pagesA Patient With PalpitationChris Jardine LiNo ratings yet
- EcgDocument34 pagesEcgSundara Rami ReddyNo ratings yet
- DR Jess Feltcher - Palpitations in General Practicce - 0Document49 pagesDR Jess Feltcher - Palpitations in General Practicce - 0aim1997No ratings yet
- Heart BlockDocument30 pagesHeart BlockM Farhad KhaniNo ratings yet
- Sugiyono, S.Kep., Ners., M.KepDocument48 pagesSugiyono, S.Kep., Ners., M.KepHervin RamadhaniNo ratings yet
- EKG Presentation Nov 2020Document74 pagesEKG Presentation Nov 2020AUH ICUNo ratings yet
- Bls and Acls: Deepika SelvaDocument82 pagesBls and Acls: Deepika SelvaPriyanka TNo ratings yet
- Osce PalpitationshistoryDocument3 pagesOsce PalpitationshistoryEvan O'FlahertyNo ratings yet
- Advanced Cardiac Life Support (ACLS) : By: Diana Blum MSN Metropolitan Community College Nursing 2150Document16 pagesAdvanced Cardiac Life Support (ACLS) : By: Diana Blum MSN Metropolitan Community College Nursing 2150Vikneswara SoorianarayananNo ratings yet
- An Approach To ECGDocument42 pagesAn Approach To ECGGIST (Gujarat Institute of Science & Technology)No ratings yet
- ACLS SubhankarDocument87 pagesACLS SubhankarMarc Andreo MalalaNo ratings yet
- 9 - The Cardiovascular AssessmentDocument54 pages9 - The Cardiovascular Assessmente.mb275No ratings yet
- Acls Review 2015Document29 pagesAcls Review 2015JB Reyes100% (2)
- Problem 1: Julita Suhardi Emergency Medicine BlockDocument94 pagesProblem 1: Julita Suhardi Emergency Medicine BlockZhul Thaa PurpleholicNo ratings yet
- Core Clerkship Review - RRR v4Document140 pagesCore Clerkship Review - RRR v4Kelvin ZhouNo ratings yet
- Cardiac Arrest of MedicinesDocument38 pagesCardiac Arrest of MedicinesAtirah AaNo ratings yet
- Advanced Life SupportDocument65 pagesAdvanced Life SupportHandrian RahmanNo ratings yet
- CNS M1 Lecture Slides Compiled, DR OsaiDocument185 pagesCNS M1 Lecture Slides Compiled, DR OsaiMusaNo ratings yet
- Ecg Reading PresntDocument101 pagesEcg Reading PresntbasilielnasirNo ratings yet
- Lecture - 15.arrhythmiasDocument45 pagesLecture - 15.arrhythmiasMohammed A MalkawiNo ratings yet
- Exercise Stress TestDocument22 pagesExercise Stress Testafrin nirfaNo ratings yet
- Stable Ischemic HeartDocument217 pagesStable Ischemic HeartReda SoNo ratings yet
- L2 ECG Monitoring I Moodle - 2023Document64 pagesL2 ECG Monitoring I Moodle - 2023Hailey YanNo ratings yet
- DIAGNOSTIC EXAM - Prof QuintosDocument12 pagesDIAGNOSTIC EXAM - Prof Quintoserjen gamingNo ratings yet
- Cardiac Arrest1Document27 pagesCardiac Arrest1Muhammad HaekalNo ratings yet
- Cardiac Rhythm and Related Disorders: - Marshell Tendean, MD - Department of Internal Medicine UKRIDA JakartaDocument50 pagesCardiac Rhythm and Related Disorders: - Marshell Tendean, MD - Department of Internal Medicine UKRIDA JakartavaiyenNo ratings yet
- PacemakerDocument63 pagesPacemakerMonish RautNo ratings yet
- 20 Blok 15 Tahun 2015 SVT DysrrhytmiasDocument69 pages20 Blok 15 Tahun 2015 SVT Dysrrhytmiaswarriordc1995No ratings yet
- 28b - EMRCOG SUMMARY - STROKE IN PREGNANCY - TOG 2020Document8 pages28b - EMRCOG SUMMARY - STROKE IN PREGNANCY - TOG 2020saeed hasan saeedNo ratings yet
- MP 20-30-40!50!60 70 90 Rel. B.1 IntelliVue Patient Monitor - Configuration ... PDF Nodeid 584073&vernum 1Document130 pagesMP 20-30-40!50!60 70 90 Rel. B.1 IntelliVue Patient Monitor - Configuration ... PDF Nodeid 584073&vernum 1Juan AmaroNo ratings yet
- Long-Term Outcome After Catheter Ablation of Ventricular Tachycardia in Patients With Nonischemic Dilated CardiomyopathyDocument11 pagesLong-Term Outcome After Catheter Ablation of Ventricular Tachycardia in Patients With Nonischemic Dilated CardiomyopathySteve MurrayNo ratings yet
- ArrestDocument9 pagesArrestBimaIndraNo ratings yet
- Use of Simulation Based Medical Education For AdvaDocument4 pagesUse of Simulation Based Medical Education For AdvaLê Huy HoàngNo ratings yet
- Asystole: Ventricular FibrillationDocument3 pagesAsystole: Ventricular FibrillationLucia CorlatNo ratings yet
- Advanced ECG AnalysisDocument90 pagesAdvanced ECG AnalysisnursewinstonNo ratings yet
- iGA Iforia-ProMRI Mul 393471-J 2017-11-24 EsDocument76 pagesiGA Iforia-ProMRI Mul 393471-J 2017-11-24 EsMartin ArrietaNo ratings yet
- Comprehensive Edited)Document82 pagesComprehensive Edited)mikrobyo_ng_wmsuNo ratings yet
- Rhythms of Death MD1TALKDocument1 pageRhythms of Death MD1TALKAmalNo ratings yet
- Acls AllDocument71 pagesAcls Allezzat salemNo ratings yet
- FREE 2021 ACLS Study Guide - ACLS Made Easy!Document32 pagesFREE 2021 ACLS Study Guide - ACLS Made Easy!Alen ArguellesNo ratings yet
- Paper 3Document10 pagesPaper 3Ahmed AlrefaiNo ratings yet
- Als Protocol Dec 2023 FinalDocument84 pagesAls Protocol Dec 2023 FinalRobert MccallumNo ratings yet
- Arrhythmogenic Left Ventricular CardiomyopathyDocument11 pagesArrhythmogenic Left Ventricular CardiomyopathyCristian urrutia castilloNo ratings yet
- Ehra Position Paper: Europace (2018) 20, 1719-1720 Doi:10.1093/europace/eux380Document35 pagesEhra Position Paper: Europace (2018) 20, 1719-1720 Doi:10.1093/europace/eux380Karen OezauNo ratings yet