You might also like
- Harris Et Al. (2004) - Diagnosis and Treatment of Pediatric FlatfootDocument33 pagesHarris Et Al. (2004) - Diagnosis and Treatment of Pediatric FlatfootxtraqrkyNo ratings yet
- Early Detection of Pediatric Orthopedic DisordersDocument35 pagesEarly Detection of Pediatric Orthopedic Disordersdina hapsariNo ratings yet
- Amor Fati Principles for Self-Mastery in 30 StepsDocument2 pagesAmor Fati Principles for Self-Mastery in 30 StepsG. Gordon LiddyNo ratings yet
- 04-Locked Plate Fixation - Principle and ApplicationsDocument67 pages04-Locked Plate Fixation - Principle and Applicationsb2v9999No ratings yet
- The Alice Network: A Novel by Kate Quinn | Conversation StartersFrom EverandThe Alice Network: A Novel by Kate Quinn | Conversation StartersNo ratings yet
- Gold Etf: Presented byDocument16 pagesGold Etf: Presented byAjay YadavNo ratings yet
- Agnes Callard On The Last GenerationDocument4 pagesAgnes Callard On The Last GenerationVivek BalramNo ratings yet
- How To Read A Postoperative Knee Replacement RadiographDocument9 pagesHow To Read A Postoperative Knee Replacement RadiographNegru TeodorNo ratings yet
- Presented By: DR Venkatesh V Moderator: DR Harish KDocument81 pagesPresented By: DR Venkatesh V Moderator: DR Harish KPankaj VatsaNo ratings yet
- Chapter 21: Surgery of The Congenital FootDocument30 pagesChapter 21: Surgery of The Congenital FootpoddataNo ratings yet
- Total Knee Replacement GuideDocument27 pagesTotal Knee Replacement GuideMuiz SaddozaiNo ratings yet
- MOC Notes 2011 NewDocument181 pagesMOC Notes 2011 NewMohit GuptaNo ratings yet
- OsteotomyDocument4 pagesOsteotomyMihai DuduNo ratings yet
- Limited Rotation of The 3-44Document6 pagesLimited Rotation of The 3-44HAKAN PARNo ratings yet
- Shoulder Arthroplasty WIC - Dr. LSDocument56 pagesShoulder Arthroplasty WIC - Dr. LSDifitasari Cipta Perdana100% (1)
- Knee Joint Materials and Components: by M.L. Stills, C ODocument4 pagesKnee Joint Materials and Components: by M.L. Stills, C OSusan KNo ratings yet
- Hemipelvectomy and hip disarticulation proceduresDocument40 pagesHemipelvectomy and hip disarticulation proceduresCarmelle Zia ReyesNo ratings yet
- Splints BracesDocument18 pagesSplints BracesvaishnaviNo ratings yet
- Lower Extremity Socket Design and Suspension: Kevin Carroll, MS, CP, FAAOPDocument18 pagesLower Extremity Socket Design and Suspension: Kevin Carroll, MS, CP, FAAOPMatthew PhillipsNo ratings yet
- Closing Wedge Osteotomy of The Tibia and The FemurDocument12 pagesClosing Wedge Osteotomy of The Tibia and The Femuralyek92No ratings yet
- Chapter 19Document25 pagesChapter 19MuhammadMusa47No ratings yet
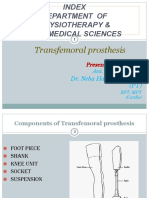
- TRANSFEMORAL - PPT 1Document64 pagesTRANSFEMORAL - PPT 1Farheen KhanNo ratings yet
- UCBL LectureDocument29 pagesUCBL Lectureergosadia658No ratings yet
- THR Dan TKRDocument122 pagesTHR Dan TKRAdi ShdbNo ratings yet
- JessDocument20 pagesJessdeepaliarneja67% (3)
- Patellofemoral Pain After Total Knee Arthroplasty PDFDocument8 pagesPatellofemoral Pain After Total Knee Arthroplasty PDFSergiu PlescaNo ratings yet
- KAFO and KO Guide for Lower Limb StabilizationDocument35 pagesKAFO and KO Guide for Lower Limb StabilizationMaryam KhalidNo ratings yet
- jkhs-21-202 Ko enDocument9 pagesjkhs-21-202 Ko enlaurenNo ratings yet
- 1 s2.0 S089184220200054X Main PDFDocument32 pages1 s2.0 S089184220200054X Main PDFAnonymous kdBDppigENo ratings yet
- Biomechanics of ArthroplastyDocument57 pagesBiomechanics of ArthroplastyUsama RafiqNo ratings yet
- Medical Management of DDHDocument5 pagesMedical Management of DDHMark Christian CuiNo ratings yet
- Knee ReplacementDocument2 pagesKnee ReplacementpahumbleNo ratings yet
- 2014 Article 9237Document6 pages2014 Article 9237Mahmoud A KhatabNo ratings yet
- The Evolution of Total Knee ReplacementDocument82 pagesThe Evolution of Total Knee ReplacementMihaela DoniciNo ratings yet
- Total Knee Replacement Prosthesis AssignmentDocument33 pagesTotal Knee Replacement Prosthesis Assignmentdr neha gaggarNo ratings yet
- Surgical Treatment of ClubfootDocument49 pagesSurgical Treatment of Clubfootvishwas dabasNo ratings yet
- (Literally "Re-Forming of Joint") : ArthroplastyDocument93 pages(Literally "Re-Forming of Joint") : ArthroplastykotraeNo ratings yet
- Sto Indus Knee 2Document59 pagesSto Indus Knee 2Purushothama Rao NalamatiNo ratings yet
- Mitek Anchor SurgeryDocument9 pagesMitek Anchor SurgeryHeidy IxcaraguaNo ratings yet
- Ankle Disarticulation Prosthetics: Course Work ManualDocument52 pagesAnkle Disarticulation Prosthetics: Course Work ManualJananthan Thavarajah67% (3)
- PONSETTI METHOD FOR CLUBFOOT CORRECTIONDocument5 pagesPONSETTI METHOD FOR CLUBFOOT CORRECTIONIjaz KhanNo ratings yet
- Mathew 2017Document12 pagesMathew 2017Negru TeodorNo ratings yet
- Foot Orthosis and Lower Limb Bracing GuideDocument25 pagesFoot Orthosis and Lower Limb Bracing GuideAbdul Al-FattahNo ratings yet
- Distal Femoral Locking Plates For Tibiotalocalcaneal Fusions in The Charcot Ankle: A Retrospective StudyDocument6 pagesDistal Femoral Locking Plates For Tibiotalocalcaneal Fusions in The Charcot Ankle: A Retrospective StudybaoNo ratings yet
- Gait Patterns in Individuals With AmputationDocument7 pagesGait Patterns in Individuals With AmputationSangeetha GnaneswaranNo ratings yet
- The Neurophysiological Ankle Foot OrthosisDocument32 pagesThe Neurophysiological Ankle Foot OrthosisSanket RoutNo ratings yet
- Conferences and Reviews Total Hip Arthroplasty: or An A ReconDocument7 pagesConferences and Reviews Total Hip Arthroplasty: or An A ReconSekar CitrasariNo ratings yet
- Solomon 2010Document10 pagesSolomon 2010Roger WatersNo ratings yet
- Evaluation Procedures For Lower Limb OrthosesDocument19 pagesEvaluation Procedures For Lower Limb OrthosesMaryam KhalidNo ratings yet
- Aaos2007 Hip Knee PDFDocument61 pagesAaos2007 Hip Knee PDFHéctor Pando SánchezNo ratings yet
- InTech-Posterior Stabilized Total Knee ArthroplastyDocument12 pagesInTech-Posterior Stabilized Total Knee ArthroplastyfranciscoNo ratings yet
- Knee ReplacementDocument7 pagesKnee ReplacementChandan Kumar ChoubeyNo ratings yet
- Knee MobilebearingkneeDocument20 pagesKnee MobilebearingkneeJobin VargheseNo ratings yet
- ORTHOTIC BASICSDocument94 pagesORTHOTIC BASICSAkbar AziziNo ratings yet
- Kogler 1996Document10 pagesKogler 1996David LiNo ratings yet
- Calcaneo StopDocument5 pagesCalcaneo StoppecheniqNo ratings yet
- Prosthesis: Presented by Dr. Chiranjeevi.JDocument63 pagesProsthesis: Presented by Dr. Chiranjeevi.JchirusdunnaNo ratings yet
- PFFD (Proximal Femoral Focal Deficiency)Document19 pagesPFFD (Proximal Femoral Focal Deficiency)RaviKumarNo ratings yet
- Joshis External Stabilisation System Jess For Recurrent Ctev Due To Irregular Follow Up PDFDocument5 pagesJoshis External Stabilisation System Jess For Recurrent Ctev Due To Irregular Follow Up PDFshankarNo ratings yet
- ArthroplastyDocument64 pagesArthroplastyAmit Kochhar75% (4)
- BPH Seminar Nursing Care GuideDocument19 pagesBPH Seminar Nursing Care GuideHoney PrasadNo ratings yet
- Digestive Disorders April 2007 PDFDocument8 pagesDigestive Disorders April 2007 PDFAnanta RanaNo ratings yet
- Health Assessment Exam 1 Study GuideDocument8 pagesHealth Assessment Exam 1 Study GuideDharati Patel100% (1)
- Zirconia ImplantsDocument15 pagesZirconia ImplantsmusatiiNo ratings yet
- PT of The Shoulder PDFDocument573 pagesPT of The Shoulder PDFMuhammad Salman AzimNo ratings yet
- Bleomycin Monograph 1dec2014Document10 pagesBleomycin Monograph 1dec2014cmeytasNo ratings yet
- Case Group 1Document10 pagesCase Group 1JASMEEN RAVALNo ratings yet
- BSSP Course DescriptionsDocument3 pagesBSSP Course DescriptionsJilliane LagusNo ratings yet
- Stefan Et Al-2019-Journal of Clinical PsychologyDocument16 pagesStefan Et Al-2019-Journal of Clinical PsychologyYuni Indriani RombeNo ratings yet
- CPAP ManualDocument43 pagesCPAP ManualTachira Julher RiveraNo ratings yet
- Absen Metod!!!Document4 pagesAbsen Metod!!!Haris Pratama RebornNo ratings yet
- AmenorrheaDocument41 pagesAmenorrheaDewi Felayati Gusni100% (2)
- BC DENTISTS-Abbreviated Fee GuideDocument2 pagesBC DENTISTS-Abbreviated Fee Guidewilliam_V_LeeNo ratings yet
- Nutrition Support in The Hospital Patient: David Armstrong November 2, 2005Document40 pagesNutrition Support in The Hospital Patient: David Armstrong November 2, 2005Larasati HasaptiasNo ratings yet
- Personal Trainer Magazine PDFDocument54 pagesPersonal Trainer Magazine PDFdixieakerszNo ratings yet
- Acute PancreatitisDocument46 pagesAcute PancreatitisLew NianNo ratings yet
- DKADocument64 pagesDKAAravindhan Gunasekaran PaediatricianNo ratings yet
- Amenorrhea - Algorithm & DifferentialsDocument9 pagesAmenorrhea - Algorithm & DifferentialsItharshan IndreswaranNo ratings yet
- Cultivation of Super Food Spirulina Blue-Green Algae An AgribusinessDocument8 pagesCultivation of Super Food Spirulina Blue-Green Algae An AgribusinessRupesh Kumar100% (1)
- Jung's Collected WorksDocument6 pagesJung's Collected WorkskarinadapariaNo ratings yet
- AyurvedaDocument8 pagesAyurvedaAnand KumarNo ratings yet
- Intro To Pharmacology Study GuideDocument93 pagesIntro To Pharmacology Study GuideMichelle Morgan LongstrethNo ratings yet
- Care of New BornDocument25 pagesCare of New BornNirupama KsNo ratings yet
- Postpartum HaemorrhageDocument19 pagesPostpartum HaemorrhageJonas Marvin AnaqueNo ratings yet
- Chiba 2018Document9 pagesChiba 2018Fred MeyerNo ratings yet
- Being Afraid: Everyday WorriesDocument10 pagesBeing Afraid: Everyday Worriesdina171279No ratings yet
- Ultrasound ImagingDocument11 pagesUltrasound ImagingFikret Baz100% (1)
- Jurnal AnemiaDocument4 pagesJurnal AnemiaAchmad Aidil TazakkaNo ratings yet
- FAQ Updated Must Read For Apple Therapy-9Document23 pagesFAQ Updated Must Read For Apple Therapy-9dpparkheNo ratings yet
- An Update On The Management of Endometrial HyperplasiaDocument5 pagesAn Update On The Management of Endometrial Hyperplasiafitrah fajrianiNo ratings yet