You might also like
- Thyphoid FeverDocument66 pagesThyphoid FeverPurnamandala Abu FarisNo ratings yet
- Typhoid Fever Diagnosis and TreatmentDocument52 pagesTyphoid Fever Diagnosis and TreatmentOsama HassanNo ratings yet
- Typhoid Fever Pathogenesis and TreatmentDocument71 pagesTyphoid Fever Pathogenesis and TreatmentDionisius KevinNo ratings yet
- 04 - Typhoid FeverDocument31 pages04 - Typhoid FeverGloria MachariaNo ratings yet
- Typhoid Fever PPT 30-3-10Document97 pagesTyphoid Fever PPT 30-3-10Anonymous hYMWbA100% (1)
- 04 - Typhoid FeverDocument35 pages04 - Typhoid Feversoheil100% (1)
- Typhoid FeverDocument46 pagesTyphoid Feverdeskichinta50% (2)
- 伤寒英文教案 Typhoid Fever-应若素Document36 pages伤寒英文教案 Typhoid Fever-应若素Wai Kwong ChiuNo ratings yet
- Enteric VikrannthDocument71 pagesEnteric Vikrannthvikrannth vNo ratings yet
- Typhoid and Paratyphoid Fever GuideDocument70 pagesTyphoid and Paratyphoid Fever GuideAnwar SolihinNo ratings yet
- Demam Tifoid: Sigit Widyatmoko Fakultas Kedokteran Universitas Muhammadiyah SurakartaDocument37 pagesDemam Tifoid: Sigit Widyatmoko Fakultas Kedokteran Universitas Muhammadiyah SurakartasakyaNo ratings yet
- Enteric FeverDocument7 pagesEnteric FeverkudzaimuregidubeNo ratings yet
- Acute Febrile IllnessesDocument54 pagesAcute Febrile IllnessesfraolNo ratings yet
- A Sacrifice to Become A Doctor: 18-Year-Old Student's Medical StruggleDocument47 pagesA Sacrifice to Become A Doctor: 18-Year-Old Student's Medical StruggleEric RicardoNo ratings yet
- DRAFT TM CASE 2: Typhoid FeverDocument7 pagesDRAFT TM CASE 2: Typhoid FeverIno HajrinNo ratings yet
- Typhoid Fever: by Dr. Bambang SN, SP - PD Department of Internal Medicine, General Hospital of Dr. Soedarso, PontianakDocument32 pagesTyphoid Fever: by Dr. Bambang SN, SP - PD Department of Internal Medicine, General Hospital of Dr. Soedarso, PontianakTriponiaNo ratings yet
- Problem 3 - VarlaDocument75 pagesProblem 3 - VarlavarlavarleyNo ratings yet
- Salmonellosis LectureDocument19 pagesSalmonellosis LectureEslam HamadaNo ratings yet
- Typhoid Fever: Dept. Infectious Disease 2nd Affiliated Hospital CMUDocument23 pagesTyphoid Fever: Dept. Infectious Disease 2nd Affiliated Hospital CMUAidil Fittriani AyuNo ratings yet
- Enteric FeverDocument20 pagesEnteric FeverLusi UtamiNo ratings yet
- Surgical Complication of Typhoid FeverDocument10 pagesSurgical Complication of Typhoid FeverHelsa Eldatarina JNo ratings yet
- TyphoidDocument26 pagesTyphoidLiya Mary ThomasNo ratings yet
- Demam TifoidDocument106 pagesDemam TifoidMasYurahNharaBarusNo ratings yet
- Typhoid FeverDocument9 pagesTyphoid FeverAli Al.JuffairiNo ratings yet
- Articles English TyphoidDocument13 pagesArticles English TyphoidSiDewiAjja100% (1)
- 1.3 Demam Tifoid Dan Kelainan HeparDocument145 pages1.3 Demam Tifoid Dan Kelainan HeparajikwaNo ratings yet
- DENGUE CONTROL PROGRAM: Prevention, Symptoms, TreatmentDocument23 pagesDENGUE CONTROL PROGRAM: Prevention, Symptoms, TreatmentERMIAS, ZENDY I.No ratings yet
- Pa Tho Physiology of Typhoid Fever and Acute GastroenteritisDocument4 pagesPa Tho Physiology of Typhoid Fever and Acute GastroenteritisJade Fatima D. CaymoNo ratings yet
- Hepatitis: An Inflammation of the LiverDocument92 pagesHepatitis: An Inflammation of the Livermuhammad dimasNo ratings yet
- Shigella - Режим Совместимости - ВосстановленDocument25 pagesShigella - Режим Совместимости - Восстановленabbassi mohammedNo ratings yet
- Communicable Diseases - AntiponaDocument79 pagesCommunicable Diseases - AntiponaRegie de JesusNo ratings yet
- Feco-orally Transmitted DiseasesDocument133 pagesFeco-orally Transmitted DiseasesTekletsadikNo ratings yet
- Communicable Diseases: Roberto M. Salvador Jr. R.N.,M.D. Infectious and Tropical Disease SpecialistDocument846 pagesCommunicable Diseases: Roberto M. Salvador Jr. R.N.,M.D. Infectious and Tropical Disease SpecialistGrn Mynjrkxz100% (1)
- Typhoid Fever: Dr. Ahmad Fariz Malvi Zamzam Zein, SP - PD Departemen Ilmu Penyakit Dalam RSUD Waled - FK UnswagatiDocument19 pagesTyphoid Fever: Dr. Ahmad Fariz Malvi Zamzam Zein, SP - PD Departemen Ilmu Penyakit Dalam RSUD Waled - FK UnswagatiHary SaktiawanNo ratings yet
- Typhoid Fever WordDocument4 pagesTyphoid Fever WordfernandoNo ratings yet
- Acute GastroenteritisDocument35 pagesAcute GastroenteritisAdil ShabbirNo ratings yet
- L15 SalmonellaDocument19 pagesL15 SalmonellaMohammed RedhaNo ratings yet
- Typhoid FeverDocument27 pagesTyphoid FeverDonn Alcayde100% (2)
- Typhoid Fever: Infectious DiseaseDocument18 pagesTyphoid Fever: Infectious DiseaseSoumyadip PradhanNo ratings yet
- TyphoidDocument13 pagesTyphoidMayuri VohraNo ratings yet
- Report On Etiology, Epidemiology, Clinic, DD, Treatment, Profilaxis of Typhoid Fever & ParathyphoidDocument3 pagesReport On Etiology, Epidemiology, Clinic, DD, Treatment, Profilaxis of Typhoid Fever & ParathyphoidAdnan Akram, MD (Latvia)No ratings yet
- Typhoid Fever: (Enterica)Document22 pagesTyphoid Fever: (Enterica)Mans FansNo ratings yet
- CURA Mono, Rheu, HyperDocument89 pagesCURA Mono, Rheu, Hyperwiwi_13No ratings yet
- Typhoid FeverDocument52 pagesTyphoid Fevertummalapalli venkateswara rao100% (5)
- Salmonella Infections: (Salmonelloses)Document56 pagesSalmonella Infections: (Salmonelloses)andualemNo ratings yet
- Typhoid FeverDocument5 pagesTyphoid FeverNaziha InaamNo ratings yet
- Typhoid Fever Case Presenting with Multiple ComplicationsDocument4 pagesTyphoid Fever Case Presenting with Multiple ComplicationsCleo CaminadeNo ratings yet
- Enteric Fever: Causes, Symptoms, Diagnosis & TreatmentDocument2 pagesEnteric Fever: Causes, Symptoms, Diagnosis & TreatmentAjay Pal NattNo ratings yet
- L1tojl Ophcu) bq8fDocument31 pagesL1tojl Ophcu) bq8fKristel AnneNo ratings yet
- Salmonella Typhi and Salmonella Paratyphi Are The Causative Agents of Typhoid FeverDocument15 pagesSalmonella Typhi and Salmonella Paratyphi Are The Causative Agents of Typhoid FeverfitrianugrahNo ratings yet
- Typhoid FeverDocument24 pagesTyphoid FeverHazielle BondocNo ratings yet
- Referat Demam TifoidDocument30 pagesReferat Demam TifoidBening IrhamnaNo ratings yet
- Typhoid Fever (Enteric Fever)Document24 pagesTyphoid Fever (Enteric Fever)Liza Marie Cayetano AdarneNo ratings yet
- GI Infections of Small Bowel and Colon Chapter 11 Ddsep9Document105 pagesGI Infections of Small Bowel and Colon Chapter 11 Ddsep9Hima AlqahtaniNo ratings yet
- Portal Vein Thrombosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPortal Vein Thrombosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Female Urinary Tract Infections in Clinical PracticeFrom EverandFemale Urinary Tract Infections in Clinical PracticeBob YangNo ratings yet
- 17oncology1 Growth Disturbances TextsDocument28 pages17oncology1 Growth Disturbances TextsDrDeepak PawarNo ratings yet
- Data Collection FormDocument2 pagesData Collection FormDrDeepak PawarNo ratings yet
- Tables and GraphsDocument17 pagesTables and GraphsDrDeepak PawarNo ratings yet
- List of FiguresDocument2 pagesList of FiguresDrDeepak PawarNo ratings yet
- Methodology DMDocument3 pagesMethodology DMDrDeepak PawarNo ratings yet
- Review LiteratureDocument23 pagesReview LiteratureDrDeepak Pawar50% (4)
- Results and DiscussionDocument5 pagesResults and DiscussionDrDeepak PawarNo ratings yet
- List of FiguresDocument2 pagesList of FiguresDrDeepak PawarNo ratings yet
- ACRONYMSDocument2 pagesACRONYMSDrDeepak PawarNo ratings yet
- Assessing Diabetes AwarenessDocument7 pagesAssessing Diabetes AwarenessDrDeepak PawarNo ratings yet
- DM Conclusion 222Document2 pagesDM Conclusion 222DrDeepak PawarNo ratings yet
- 7-Steps For DI Systematic ApproachDocument8 pages7-Steps For DI Systematic ApproachDrDeepak Pawar71% (7)
- Chapter 3 Aim and ObjectivesDocument1 pageChapter 3 Aim and ObjectivesDrDeepak PawarNo ratings yet
- INTRODUCTIONDocument5 pagesINTRODUCTIONDrDeepak PawarNo ratings yet
- Oligo Research Article PDFDocument4 pagesOligo Research Article PDFDrDeepak PawarNo ratings yet
- Antibiotics For Upper Respiratory Tract Infections: Follow-Up Utilization and Antibiotic UseDocument5 pagesAntibiotics For Upper Respiratory Tract Infections: Follow-Up Utilization and Antibiotic UseDrDeepak PawarNo ratings yet
- A Seminar On Lower Respiratory Tract Infections: Click To Edit Master Subtitle StyleDocument44 pagesA Seminar On Lower Respiratory Tract Infections: Click To Edit Master Subtitle StyleDrDeepak PawarNo ratings yet
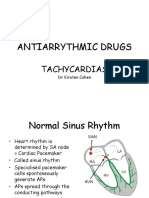
- Antiarrythmic Drugs: TachycardiasDocument36 pagesAntiarrythmic Drugs: TachycardiasDrDeepak PawarNo ratings yet
- Introduction to Toxicology Concepts and UnitsDocument40 pagesIntroduction to Toxicology Concepts and UnitsFauzan FasnidNo ratings yet
- 01 M039 43754Document16 pages01 M039 43754DrDeepak PawarNo ratings yet
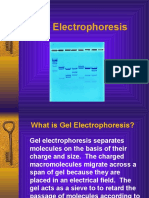
- GelelctroDocument11 pagesGelelctroDrDeepak PawarNo ratings yet
- 01 M006 36157Document12 pages01 M006 36157DrDeepak PawarNo ratings yet
- Barbiturate PoisoningDocument3 pagesBarbiturate PoisoningDrDeepak PawarNo ratings yet
- 10 2 33 PDFDocument4 pages10 2 33 PDFDrDeepak PawarNo ratings yet
- Lower Respiratory Tract Infections SeminarDocument45 pagesLower Respiratory Tract Infections SeminarDrDeepak PawarNo ratings yet
- Perbedaan Papila Dan Folikel Pada MataDocument2 pagesPerbedaan Papila Dan Folikel Pada MataMuhammad Agus Nashir100% (1)
- Expanded Program On ImmunizationDocument7 pagesExpanded Program On ImmunizationGLadys Gegare100% (1)
- Expel Mucus, Fight Respiratory Irritation With Mighty Mullein & GingerDocument8 pagesExpel Mucus, Fight Respiratory Irritation With Mighty Mullein & GingerCarl MacCordNo ratings yet
- Week 5 Past Perfect Practice 2Document4 pagesWeek 5 Past Perfect Practice 2Soldjair Mantari SotoNo ratings yet
- Molecular Virology, 2013 Edition (PDF) (DR - Carson) VRG PDFDocument1,013 pagesMolecular Virology, 2013 Edition (PDF) (DR - Carson) VRG PDFYuridia Rodríguez100% (3)
- BronchiectasisDocument16 pagesBronchiectasisRaras RavenclawwNo ratings yet
- LO Week 5 Tutorial 2Document7 pagesLO Week 5 Tutorial 2Hizkia MarlissaNo ratings yet
- Evidence-Based Guideline: Clinical Evaluation and Treatment of Transverse MyelitisDocument8 pagesEvidence-Based Guideline: Clinical Evaluation and Treatment of Transverse MyelitisAnonymous V5l8nmcSxbNo ratings yet
- DR Jaban Moore How Do I Know If I Have ParasitesDocument9 pagesDR Jaban Moore How Do I Know If I Have ParasitesViolet VioletNo ratings yet
- Kit InsertDocument8 pagesKit InsertMuhammad HamzarNo ratings yet
- Sharp Injury PreventionDocument12 pagesSharp Injury Preventionsimmi2768No ratings yet
- Barangay Monthly Inventory of Vaccinated Population 5-11Document4 pagesBarangay Monthly Inventory of Vaccinated Population 5-11Eduardo Cases100% (1)
- Vaccination in PregnancyDocument7 pagesVaccination in PregnancyNoraNo ratings yet
- Amoxicillin + Clavulanic AcidDocument37 pagesAmoxicillin + Clavulanic Acidsanish tiwariNo ratings yet
- Toxoigm ArcDocument6 pagesToxoigm Arctesteste testeNo ratings yet
- Journal Reading Survey OphtalmologyDocument17 pagesJournal Reading Survey OphtalmologynadyajondriNo ratings yet
- Nurse Np1 Board CramsheetDocument8 pagesNurse Np1 Board CramsheetZero TwoNo ratings yet
- CasestudyvaccinesDocument5 pagesCasestudyvaccinesapi-323720899No ratings yet
- UTIs Caused by Common PathogensDocument63 pagesUTIs Caused by Common PathogensdeasyahNo ratings yet
- Indian Baby Vaccination ChartDocument6 pagesIndian Baby Vaccination ChartpramitaNo ratings yet
- Parasitology (Lect #1) TransDocument2 pagesParasitology (Lect #1) TransSherlyn Giban InditaNo ratings yet
- Immunization EPI Huda 201212Document5 pagesImmunization EPI Huda 201212Aerish TupazNo ratings yet
- Pediatric Soap NoteDocument4 pagesPediatric Soap NoteAfinaMuthi50% (2)
- Dosis Obat Medis DasarDocument6 pagesDosis Obat Medis DasarJovitaNo ratings yet
- BK Virus R-Gene: The Power of True ExperienceDocument2 pagesBK Virus R-Gene: The Power of True ExperienceSachinNo ratings yet
- Coc Exam ModelDocument44 pagesCoc Exam ModelYeshi AbebeNo ratings yet
- Antigen Presentation To T LymphocytesDocument2 pagesAntigen Presentation To T Lymphocyteskep1313No ratings yet
- Lesson Plan With COMPREHENSIVE SEXUALITY EDUCATIONDocument15 pagesLesson Plan With COMPREHENSIVE SEXUALITY EDUCATIONHanna Banana100% (1)
- Detect pathogens from symptoms and lab testsDocument3 pagesDetect pathogens from symptoms and lab testsAbhishek pandeyNo ratings yet
- Anaphy Lec Sas-17Document4 pagesAnaphy Lec Sas-17Francis Steve RipdosNo ratings yet